

Seasonal risk factors for asthma exacerbations among inner-city children
- PMID: 25794658
- PMCID: PMC4461505
- DOI: 10.1016/j.jaci.2014.12.1942
Seasonal risk factors for asthma exacerbations among inner-city children
Abstract
Background: Asthma exacerbations remain common, even in children and adolescents, despite optimal medical management. Identification of host risk factors for exacerbations is incomplete, particularly for seasonal episodes.
Objective: We sought to define host risk factors for asthma exacerbations unique to their season of occurrence.
Methods: This is a retrospective analysis of patients aged 6 to 20 years who comprised the control groups of the Asthma Control Evaluation study and the Inner City Anti-IgE Therapy for Asthma study. Univariate and multivariate models were constructed to determine whether patients' demographic and historical factors, allergic sensitization, fraction of exhaled nitric oxide values, spirometric measurements, asthma control, and treatment requirements were associated with seasonal exacerbations.
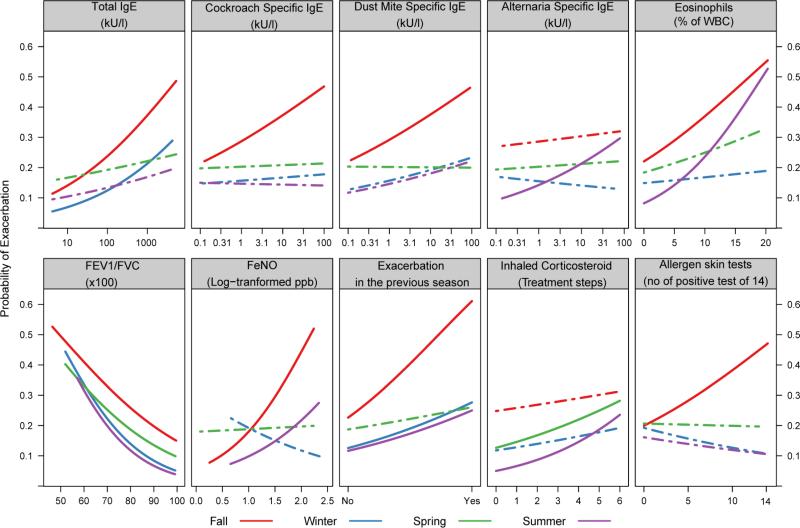
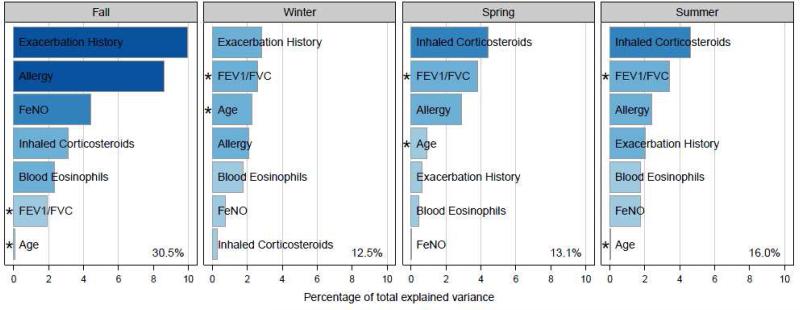
Results: The analysis included 400 patients (54.5% male; 59.0% African American; median age, 13 years). Exacerbations occurred in 37.5% of participants over the periods of observation and were most common in the fall (28.8% of participants). In univariate analysis impaired pulmonary function was significantly associated with greater odds of exacerbations for all seasons, as was an exacerbation in the previous season for all seasons except spring. In multivariate analysis exacerbation in the previous season was the strongest predictor in fall and winter, whereas a higher requirement for inhaled corticosteroids was the strongest predictor in spring and summer. The multivariate models had the best predictive power for fall exacerbations (30.5% variance attributed).
Conclusions: Among a large cohort of inner-city children with asthma, patients' risk factors for exacerbation vary by season. Thus information on individual patients might be beneficial in strategies to prevent these seasonal events.
Keywords: Asthma; IgE; allergy; asthma exacerbations; biomarkers; eosinophils; exhaled nitric oxide; pulmonary function; seasons.
Copyright © 2015 American Academy of Allergy, Asthma & Immunology. All rights reserved.
Figures
Comment in
-
Asthma exacerbations: Looking back to the future.J Allergy Clin Immunol. 2015 Jun;135(6):1474-5. doi: 10.1016/j.jaci.2015.04.013. J Allergy Clin Immunol. 2015. PMID: 26051951 No abstract available.
References
-
- Moorman JE, Akinbami LJ, Bailey CM, et al. National surveillance of asthma: United States, 2001-2010. Vital Health Stat. 2012;3:1–67. - PubMed
-
- Ivanova JI, Bergman R, Birnbaum HG, Colice GL, Silverman RA, McLaurin K. Effect of asthma exacerbations on health care costs among asthmatic patients with moderate and severe persistent asthma. The Journal of Allergy and Clinical Immunology. 2012;129:1229–35. - PubMed
-
- Sears MR. Epidemiology of asthma exacerbations. The Journal of Allergy and Clinical Immunology. 2008;122:662–8. quiz 9-70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 AI025496/AI/NIAID NIH HHS/United States
- UL1 TR001105/TR/NCATS NIH HHS/United States
- UL1 TR000451/TR/NCATS NIH HHS/United States
- UL1 RR031988/RR/NCRR NIH HHS/United States
- M01RR00071/RR/NCRR NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- 1UL1RR024156/RR/NCRR NIH HHS/United States
- HHSN272200900052C/AI/NIAID NIH HHS/United States
- HHSN272201000052I/AI/NIAID NIH HHS/United States
- UL1RR031988/RR/NCRR NIH HHS/United States
- N01-AI-25482/AI/NIAID NIH HHS/United States
- M01RR00533/RR/NCRR NIH HHS/United States
- UL1RR025741/RR/NCRR NIH HHS/United States
- UL1TR000451/TR/NCATS NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- N01 AI025482/AI/NIAID NIH HHS/United States
- M01 RR000533/RR/NCRR NIH HHS/United States
- UL1 RR024156/RR/NCRR NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- 1UL1RR025780/RR/NCRR NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- 1UL1RR025771/RR/NCRR NIH HHS/United States
- UL1 RR024982/RR/NCRR NIH HHS/United States
- RR00052/RR/NCRR NIH HHS/United States
- 5M01RR020359-04/RR/NCRR NIH HHS/United States
- N01-AI-25496/AI/NIAID NIH HHS/United States
- M01 RR020359/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
