

Pitfalls in RECIST Data Extraction for Clinical Trials: Beyond the Basics
- PMID: 25794800
- PMCID: PMC4429002
- DOI: 10.1016/j.acra.2015.01.015
Pitfalls in RECIST Data Extraction for Clinical Trials: Beyond the Basics
Abstract
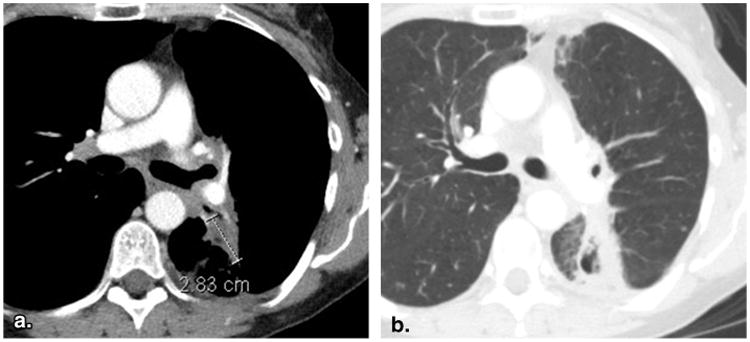
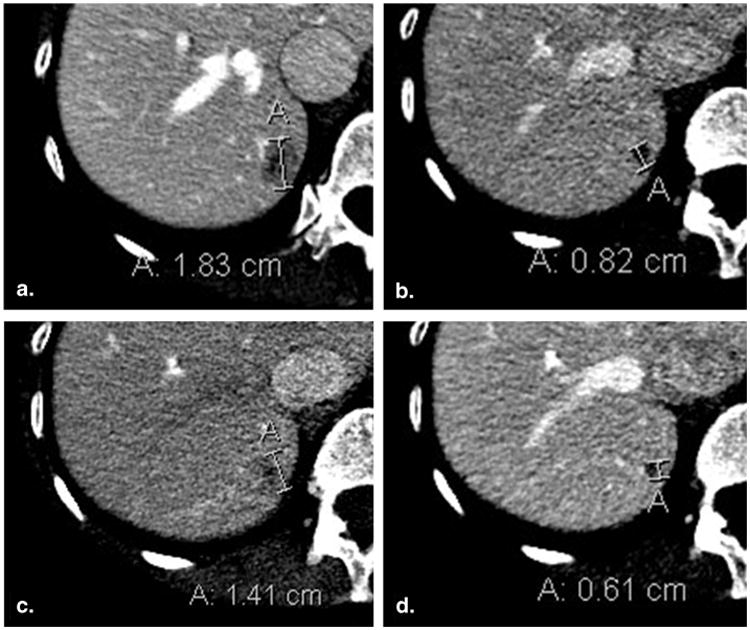
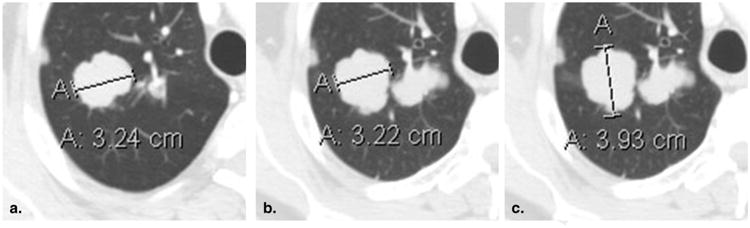
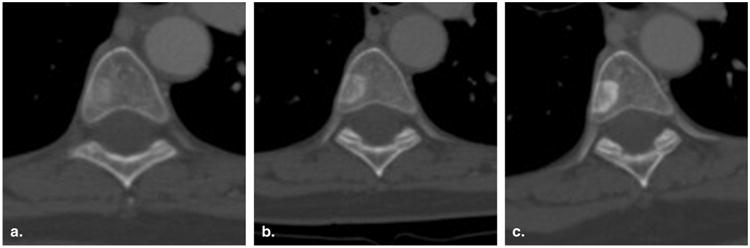
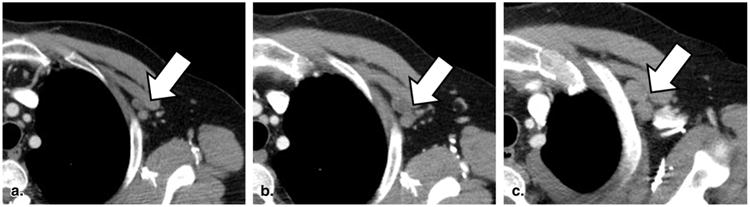
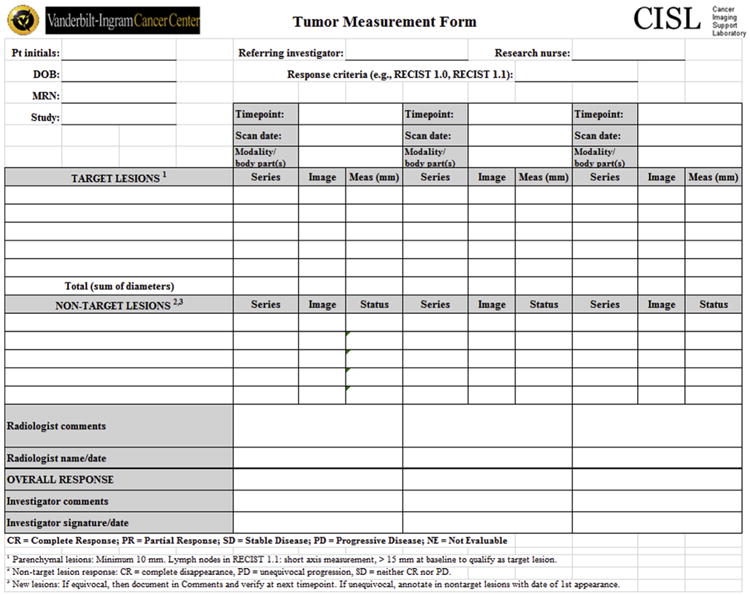
Response Evaluation Criteria in Solid Tumors (RECIST) is a standardized methodology for determining therapeutic response to anticancer therapy using changes in lesion appearance on imaging studies. Many radiologists are now using RECIST in their routine clinical workflow, as part of consultative arrangements, or within dedicated imaging core laboratories. Although basic RECIST methodology is well described in published articles and online resources, inexperienced readers may encounter difficulties with certain nuances and subtleties of RECIST. This article illustrates a set of pitfalls in RECIST assessment considered to be "beyond the basics." These pitfalls were uncovered during a quality improvement review of a recently established cancer imaging core laboratory staffed by radiologists with limited prior RECIST experience. Pitfalls are presented in four categories: (1) baseline selection of lesions, (2) reassessment of target lesions, (3) reassessment of nontarget lesions, and (4) identification of new lesions. Educational and operational strategies for addressing these pitfalls are suggested. Attention to these pitfalls and strategies may improve the overall quality of RECIST assessments performed by radiologists.
Keywords: Oncology; RECIST; antitumor efficacy; solid malignancies; tumor response assessment.
Copyright © 2015 AUR. Published by Elsevier Inc. All rights reserved.
Figures



References
-
- Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1) Eur J Cancer. 2009;45:228–247. - PubMed
-
- Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92:205–216. - PubMed
-
- Jaffe TA, Wickersham NW, Sullivan DC. Quantitative imaging in oncology patients: Part 1, radiology practice patterns at major U.S. cancer centers. AJR Am J Roentgenol. 2010;195:101–106. - PubMed
-
- Nishino M, Jagannathan JP, Ramaiya NH, et al. Revised RECIST guideline version 1.1: what oncologists want to know and what radiologists need to know. AJR Am J Roentgenol. 2010;195:281–289. - PubMed
-
- EORTC. RECIST 1.1 questions and clarifications. [Accessed January 6, 2015]; Available at: http://www.eortc.org.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
