

Peritoneal Tumorigenesis and Inflammation are Ameliorated by Humidified-Warm Carbon Dioxide Insufflation in the Mouse
- PMID: 25794828
- PMCID: PMC4687477
- DOI: 10.1245/s10434-015-4508-1
Peritoneal Tumorigenesis and Inflammation are Ameliorated by Humidified-Warm Carbon Dioxide Insufflation in the Mouse
Abstract
Background: Conventional laparoscopic surgery uses CO2 that is dry and cold, which can damage peritoneal surfaces. It is speculated that disseminated cancer cells may adhere to such damaged peritoneum and metastasize. We hypothesized that insufflation using humidified-warm CO2, which has been shown to reduce mesothelial damage, will also ameliorate peritoneal inflammation and tumor cell implantation compared to conventional dry-cold CO2.
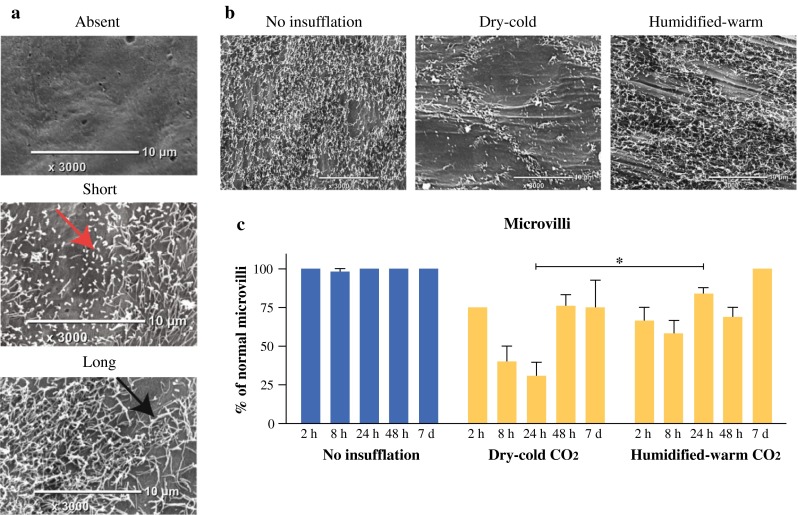
Methods: Laparoscopic insufflation was modeled in mice along with anesthesia and ventilation. Entry and exit ports were introduced to maintain insufflation using dry-cold or humidified-warm CO2 with a constant flow and pressure for 1 h; then 1000 or 1 million fluorescent-tagged murine colorectal cancer cells (CT26) were delivered into the peritoneal cavity. The peritoneum was collected at intervals up to 10 days after the procedure to measure inflammation, mesothelial damage, and tumor burden using fluorescent detection, immunohistochemistry, and scanning electron microscopy.
Results: Rapid temperature control was achieved only in the humidified-warm group. Port-site tumors were present in all mice. At 10 days, significantly fewer tumors on the peritoneum were counted in mice insufflated with humidified-warm compared to dry-cold CO2 (p < 0.03). The inflammatory marker COX-2 was significantly increased in the dry-cold compared to the humidified-warm cohort (p < 0.01), while VEGFA expression was suppressed only in the humidified-warm cohort. Significantly less mesothelial damage and tumor cell implantation was evident from 2 h after the procedure in the humidified-warm cohort.
Conclusions: Mesothelial cell damage and inflammation are reduced by using humidified-warm CO2 for laparoscopic oncologic surgery and may translate to reduce patients' risk of developing peritoneal metastasis.
Figures




References
-
- Glehen O, Kwiatkowski F, Sugarbaker PH, et al. Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. J Clin Oncol. 2004;22:3284–3292. doi: 10.1200/JCO.2004.10.012. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
