

Altered phalanx force direction during power grip following stroke
- PMID: 25795079
- PMCID: PMC4639921
- DOI: 10.1007/s00221-015-4241-9
Altered phalanx force direction during power grip following stroke
Abstract
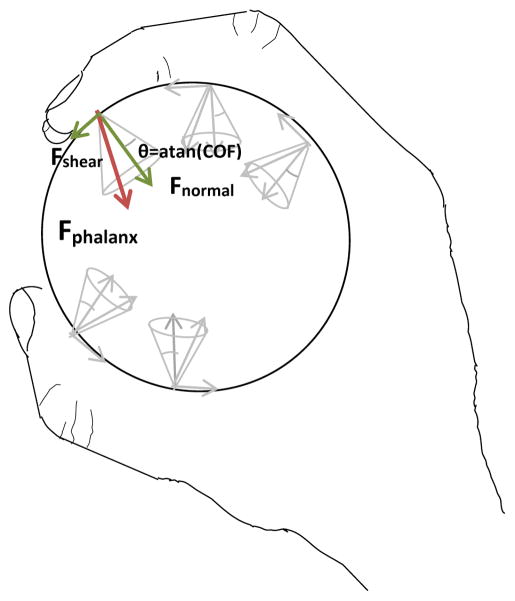
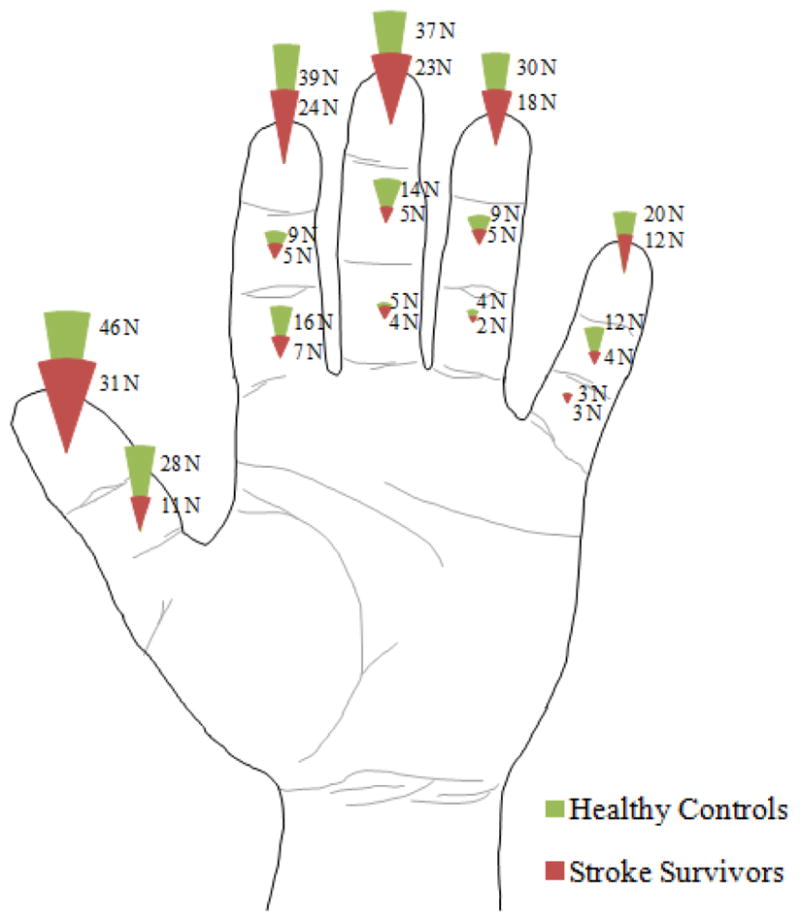
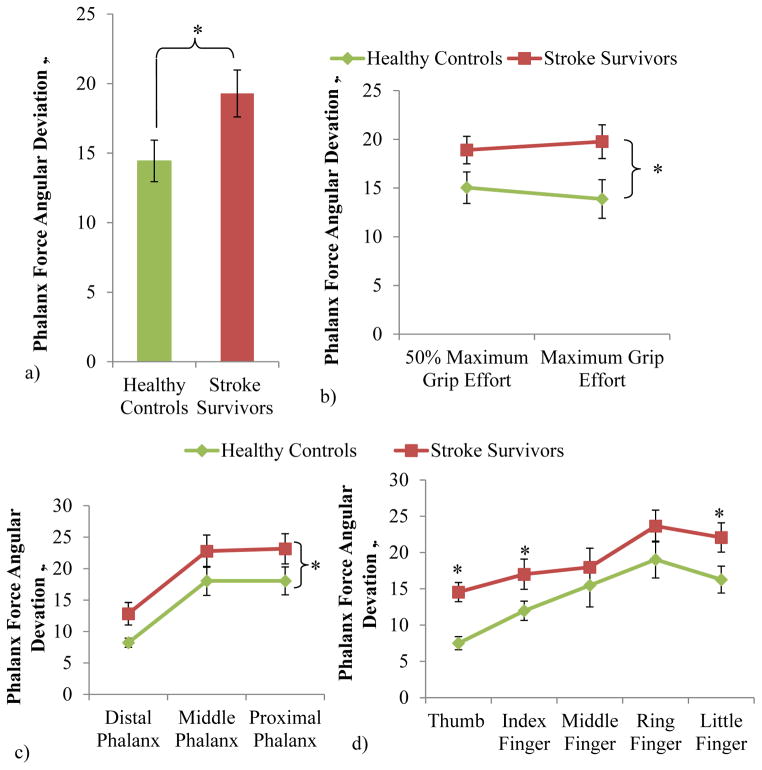
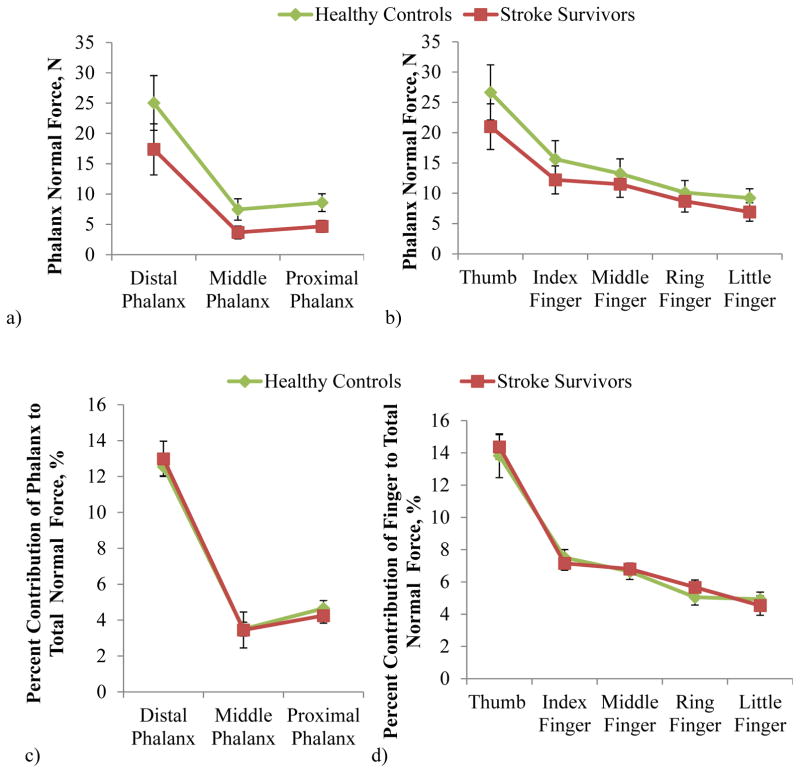
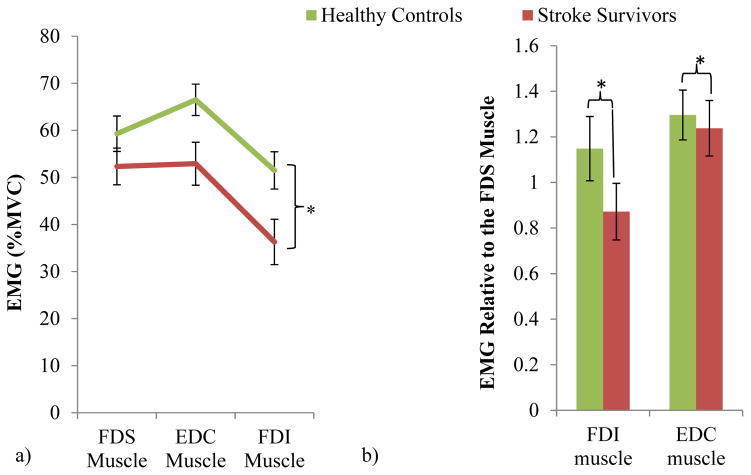
Many stroke survivors with severe impairment can grasp only with a power grip. Yet, little knowledge is available on altered power grip after stroke, other than reduced power grip strength. This study characterized stroke survivors' static power grip during 100 and 50 % maximum grip. Each phalanx force angular deviation from the normal direction and its contribution to total normal force was compared for 11 stroke survivors and 11 age-matched controls. Muscle activities and skin coefficient of friction were additionally compared for another 20 stroke and 13 age-matched control subjects. The main finding was that stroke survivors gripped with a 34 % greater phalanx force angular deviation of 19° ± 2° compared to controls of 14° ± 1° (p < .05). Stroke survivors' phalanx force angular deviation was closer to the 23° threshold of slippage between the phalanx and grip surface, which may explain increased likelihood of object dropping in stroke survivors. In addition, this altered phalanx force direction decreases normal grip force by tilting the force vector, indicating a partial role of phalanx force angular deviation in reduced grip strength post-stroke. Greater phalanx force angular deviation may biomechanically result from more severe underactivation of stroke survivors' first dorsal interosseous and extensor digitorum communis muscles compared to their flexor digitorum superficialis or somatosensory deficit. While stroke survivors' maximum power grip strength was approximately half of the controls, the distribution of their remaining strength over the fingers and phalanges did not differ, indicating evenly distributed grip force reduction over the entire hand.
Conflict of interest statement
The authors listed in this manuscript participated in the study design, collection, and preparation of the manuscript. The information conveyed in this article has not been submitted for publication elsewhere.
Figures

References
-
- Akima H, Kubo K, Imai M, Kanehisa H, Suzuki Y, Gunji A, et al. Inactivity and muscle: effect of resistance training during bed rest on muscle size in the lower limb. Acta Physiol Scand. 2001;172:269–278. - PubMed
-
- Amis AA. Variation of Finger Forces in Maximal Isometric Grasp Tests on a Range of Cylinder Diameters. Journal of Biomedical Engineering. 1987;9:313–320. - PubMed
-
- Barry BK, Carson RG. The consequences of resistance training for movement control in older adults. J Gerontol A Biol Sci Med Sci. 2004;59:730–754. - PubMed
-
- Basmajian J. Biofeedback Principles and Practice for Clinicians. Williams and Wilkins; Baltimore, MD: 1989.
-
- Blennerhassett JM, Matyas TA, Carey LM. Impaired discrimination of surface friction contributes to pinch grip deficit after stroke. Neurorehabil Neural Repair. 2007;21:263–272. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
