

Small nerve fiber quantification in the diagnosis of diabetic sensorimotor polyneuropathy: comparing corneal confocal microscopy with intraepidermal nerve fiber density
- PMID: 25795415
- PMCID: PMC4439535
- DOI: 10.2337/dc14-2422
Small nerve fiber quantification in the diagnosis of diabetic sensorimotor polyneuropathy: comparing corneal confocal microscopy with intraepidermal nerve fiber density
Abstract
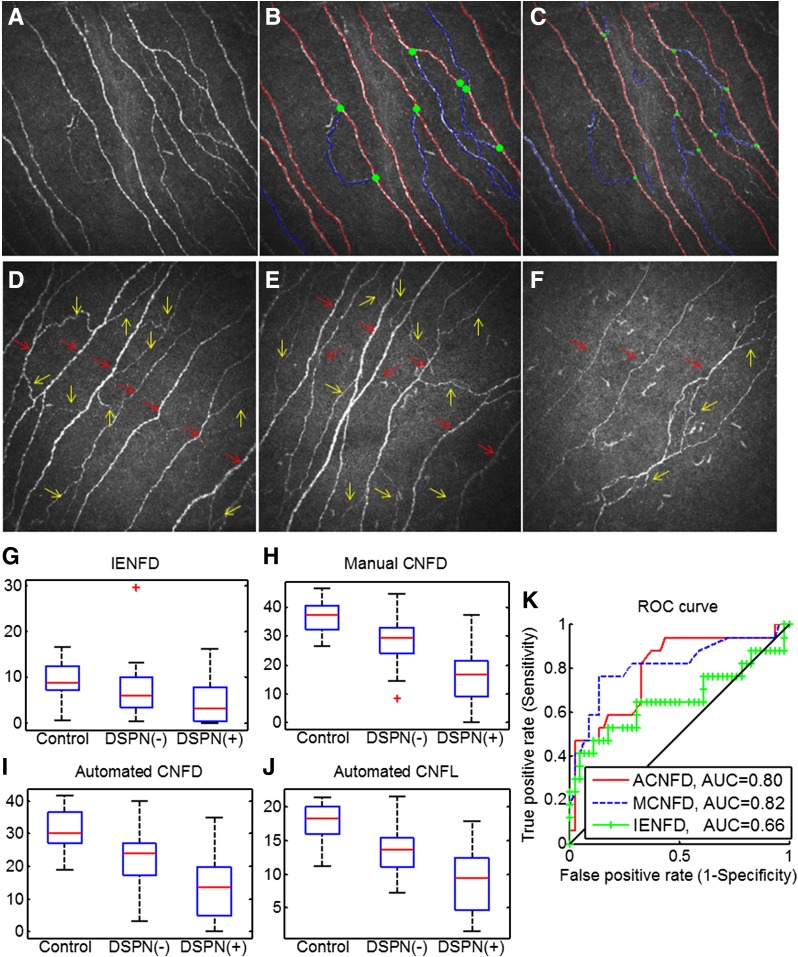
Objective: Quantitative assessment of small fiber damage is key to the early diagnosis and assessment of progression or regression of diabetic sensorimotor polyneuropathy (DSPN). Intraepidermal nerve fiber density (IENFD) is the current gold standard, but corneal confocal microscopy (CCM), an in vivo ophthalmic imaging modality, has the potential to be a noninvasive and objective image biomarker for identifying small fiber damage. The purpose of this study was to determine the diagnostic performance of CCM and IENFD by using the current guidelines as the reference standard.
Research design and methods: Eighty-nine subjects (26 control subjects and 63 patients with type 1 diabetes), with and without DSPN, underwent a detailed assessment of neuropathy, including CCM and skin biopsy.
Results: Manual and automated corneal nerve fiber density (CNFD) (P < 0.0001), branch density (CNBD) (P < 0.0001) and length (CNFL) (P < 0.0001), and IENFD (P < 0.001) were significantly reduced in patients with diabetes with DSPN compared with control subjects. The area under the receiver operating characteristic curve for identifying DSPN was 0.82 for manual CNFD, 0.80 for automated CNFD, and 0.66 for IENFD, which did not differ significantly (P = 0.14).
Conclusions: This study shows comparable diagnostic efficiency between CCM and IENFD, providing further support for the clinical utility of CCM as a surrogate end point for DSPN.
© 2015 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures
References
-
- Dyck PJ, Norell JE, Tritschler H, et al. Challenges in design of multicenter trials: end points assessed longitudinally for change and monotonicity. Diabetes Care 2007;30:2619–2625 - PubMed
-
- Malik RA. Why are there no good treatments for diabetic neuropathy? Lancet Diabetes Endocrinol 2014;2:607–609 - PubMed
-
- Boulton AJ, Kempler P, Ametov A, Ziegler D. Whither pathogenetic treatments for diabetic polyneuropathy? Diabetes Metab Res Rev 2013;29:327–333 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
