

The winding road to regenerating the human heart
- PMID: 25795463
- PMCID: PMC4430350
- DOI: 10.1016/j.carpath.2015.02.004
The winding road to regenerating the human heart
Abstract
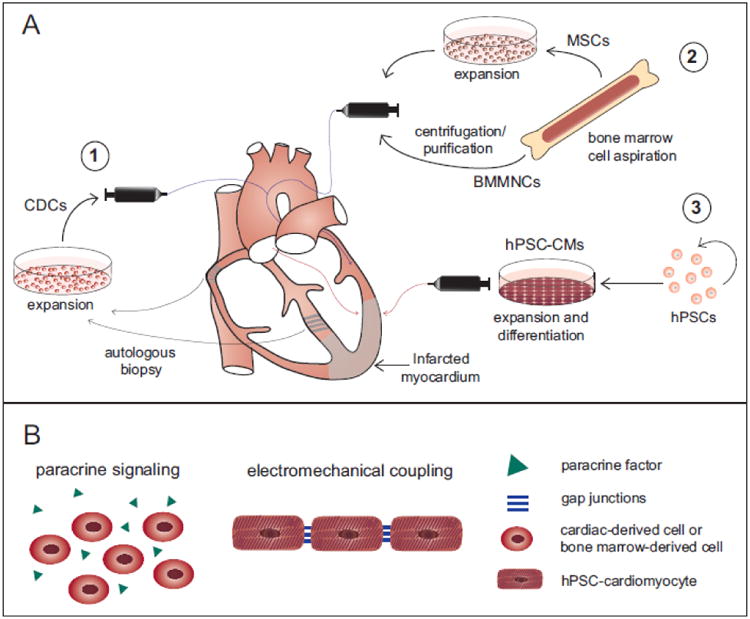
Regenerating the human heart is a challenge that has engaged researchers and clinicians around the globe for nearly a century. From the repair of the first septal defect in 1953, followed by the first successful heart transplant in 1967, and later to the first infusion of bone marrow-derived cells to the human myocardium in 2002, significant progress has been made in heart repair. However, chronic heart failure remains a leading pathological burden worldwide. Why has regenerating the human heart been such a challenge, and how close are we to achieving clinically relevant regeneration? Exciting progress has been made to establish cell transplantation techniques in recent years, and new preclinical studies in large animal models have shed light on the promises and challenges that lie ahead. In this review, we will discuss the history of cell therapy approaches and provide an overview of clinical trials using cell transplantation for heart regeneration. Focusing on the delivery of human stem cell-derived cardiomyocytes, current experimental strategies in the field will be discussed as well as their clinical translation potential. Although the human heart has not been regenerated yet, decades of experimental progress have guided us onto a promising path.
Summary: Previous work in clinical cell therapy for heart repair using bone marrow mononuclear cells, mesenchymal stem cells, and cardiac-derived cells have overall demonstrated safety and modest efficacy. Recent advancements using human stem cell-derived cardiomyocytes have established them as a next generation cell type for moving forward, however certain challenges must be overcome for this technique to be successful in the clinics.
Keywords: Cell transplantation; Heart regeneration; Myocardial infarction; Stem cell-derived cardiomyocytes.
Copyright © 2015 The Author. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Murray CJL, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet. 2012;380(9859):2197–2223. - PubMed
-
- Buja LM, Vela D. Cardiomyocyte death and renewal in the normal and diseased heart. Cardiovasc Pathol. 2008;17(6):349–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
