

Sepsis-associated acute kidney injury
- PMID: 25795495
- PMCID: PMC4507081
- DOI: 10.1016/j.semnephrol.2015.01.002
Sepsis-associated acute kidney injury
Abstract
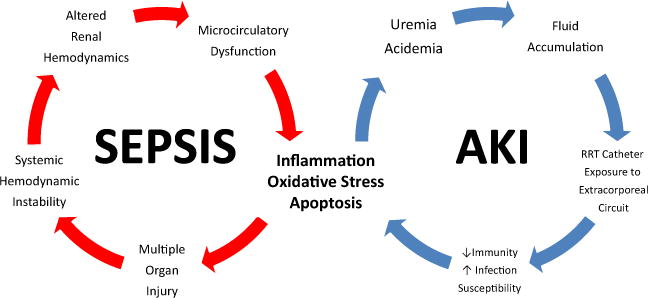
Acute kidney injury (AKI) is an epidemic problem. Sepsis has long been recognized as a foremost precipitant of AKI. Sepsis-associated AKI (SA-AKI) portends a high burden of morbidity and mortality in both children and adults with critical illness. Although our understanding of its pathophysiology is incomplete, SA-AKI likely represents a distinct subset of AKI contributed to by a unique constellation of hemodynamic, inflammatory, and immune mechanisms. SA-AKI poses significant clinical challenges for clinicians. To date, no singular effective therapy has been developed to alter the natural history of SA-AKI. Rather, current strategies to alleviate poor outcomes focus on clinical risk identification, early detection of injury, modifying clinician behavior to avoid harm, early appropriate antimicrobial therapy, and surveillance among survivors for the longer-term sequelae of kidney damage. Recent evidence has confirmed that patients no longer die with AKI, but from AKI. To improve the care and outcomes for sufferers of SA-AKI, clinicians need a robust appreciation for its epidemiology and current best-evidence strategies for prevention and treatment.
Keywords: acute kidney injury; critical care nephrology; outcomes; sepsis.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest statement: none.
Figures
References
-
- de Mendonca A, Vincent JL, Suter PM, Moreno R, Dearden NM, Antonelli M, et al. Acute renal failure in the ICU: risk factors and outcome evaluated by the SOFA score. Intensive Care Med. 2000;26:915–21. - PubMed
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S. Beginning Ending Supportive Therapy for the Kidney (B.E.S.T. Kidney) Investigators. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–8. - PubMed
-
- Ostermann M, Chang RW. Acute kidney injury in the intensive care unit according to RIFLE. Crit Care Med. 2007;35:1837–43. quiz 1852. - PubMed
-
- Bagshaw SM, George C, Dinu I, Bellomo R. A multi-centre evaluation of the RIFLE criteria for early acute kidney injury in critically ill patients. Nephrol Dial Transplant. 2008;23:1203–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
