

Long-term effects of fingolimod in multiple sclerosis: the randomized FREEDOMS extension trial
- PMID: 25795646
- PMCID: PMC4408283
- DOI: 10.1212/WNL.0000000000001462
Long-term effects of fingolimod in multiple sclerosis: the randomized FREEDOMS extension trial
Abstract
Objective: To assess long-term safety and efficacy of fingolimod in patients with relapsing-remitting multiple sclerosis (RRMS).
Methods: Patients completing FTY720 Research Evaluating Effects of Daily Oral Therapy in MS (FREEDOMS) were eligible for this dose-blinded, parallel-group extension study, continuing fingolimod 0.5 mg/day or 1.25 mg/day, or switching from placebo to either dose, randomized 1:1. Efficacy variables included annualized relapse rate (ARR), brain volume loss (BVL), and confirmed disability progression (CDP). Between-group analyses were conducted in the intent-to-treat (ITT) population from FREEDOMS baseline to end of study. Within-group analyses compared years 0-2 (FREEDOMS) and years 2-4 (extension) in the extension ITT population.
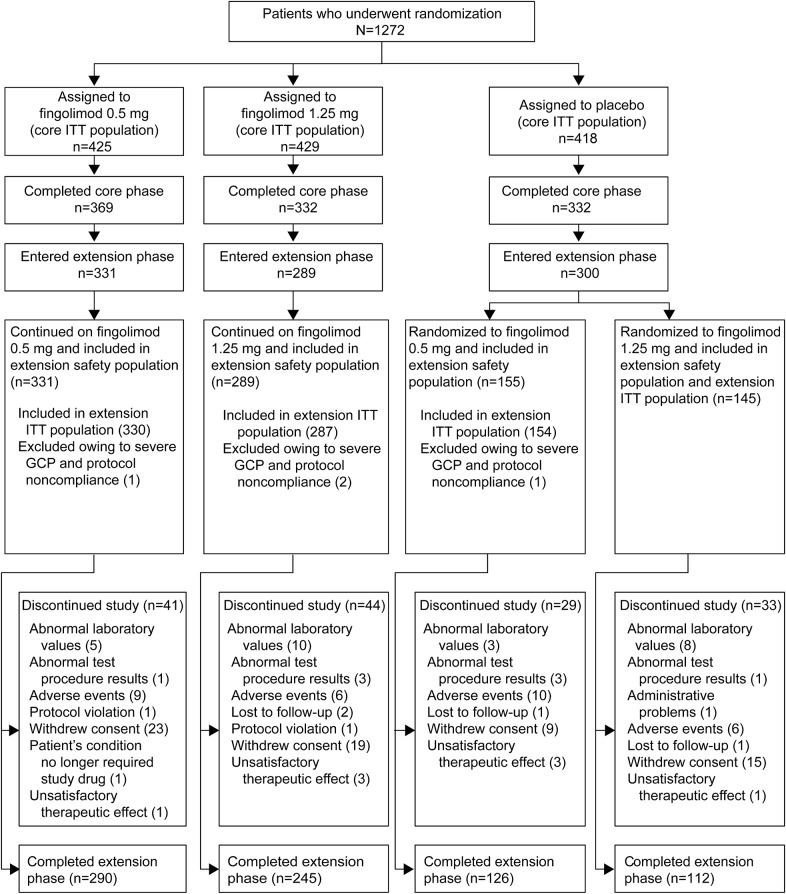
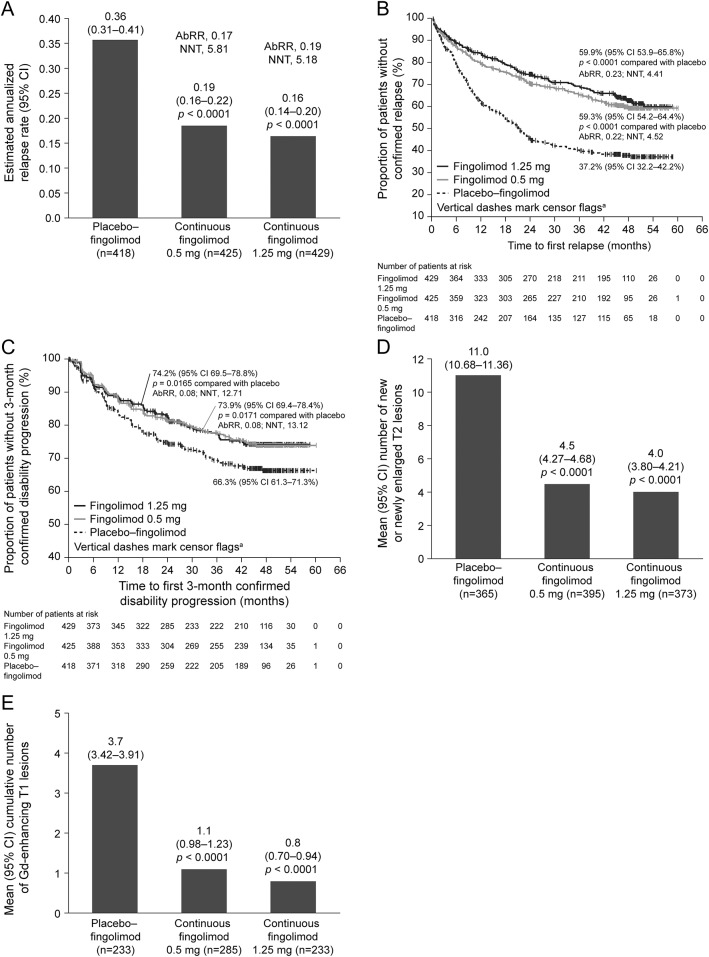
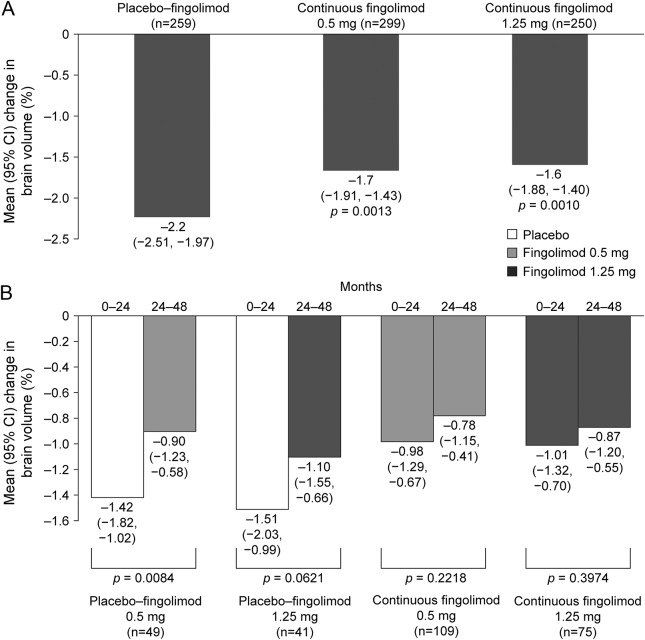
Results: Of 1,272 patients (FREEDOMS ITT population), 1,033 were eligible, and 920 enrolled in the extension study (continuous-fingolimod: 0.5 mg [n = 331], 1.25 mg [n = 289]; placebo-fingolimod: 0.5 mg [n = 155], 1.25 mg [n = 145]); 916 formed the extension ITT population (n = 330; n = 287; n = 154; n = 145) and 773 (84%) completed. In the continuous-fingolimod groups, ARR was lower (p < 0.0001), BVL was reduced (p < 0.05), and proportionately more patients were free from 3-month CDP (p < 0.05) than in a group comprising all placebo-fingolimod patients. Within each placebo-fingolimod group, ARR was lower (p < 0.001, both) and BVL was reduced after switching (p < 0.01, placebo-fingolimod 0.5 mg). Rates and types of adverse events were similar across groups; no new safety issues were reported.
Conclusion: Efficacy benefits of fingolimod during FREEDOMS were sustained during the extension; ARR and BVL were reduced after switching.
Classification of evidence: This study provides Class IV evidence that long-term fingolimod treatment is well-tolerated and reduces relapse rates, disability progression, and MRI effects in patients with RRMS.
© 2015 American Academy of Neurology.
Figures
References
-
- Brinkmann V, Davis MD, Heise CE, et al. The immune modulator FTY720 targets sphingosine 1-phosphate receptors. J Biol Chem 2002;277:21453–21457. - PubMed
-
- Cohen JA, Barkhof F, Comi G, et al. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med 2010;362:402–415. - PubMed
-
- Kappos L, Radue EW, O'Connor P, et al. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N Engl J Med 2010;362:387–401. - PubMed
-
- Calabresi PA, Radue EW, Goodin D, et al. Safety and efficacy of fingolimod in patients with relapsing-remitting multiple sclerosis (FREEDOMS II): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Neurol 2014;13:545–556. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials