

The Head Injury Retrieval Trial (HIRT): a single-centre randomised controlled trial of physician prehospital management of severe blunt head injury compared with management by paramedics only
- PMID: 25795741
- PMCID: PMC4680192
- DOI: 10.1136/emermed-2014-204390
The Head Injury Retrieval Trial (HIRT): a single-centre randomised controlled trial of physician prehospital management of severe blunt head injury compared with management by paramedics only
Abstract
Background: Advanced prehospital interventions for severe brain injury remains controversial. No previous randomised trial has been conducted to evaluate additional physician intervention compared with paramedic only care.
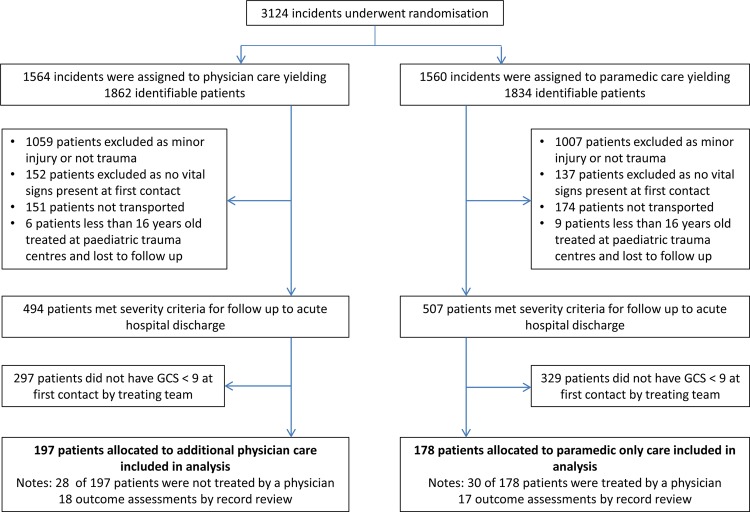
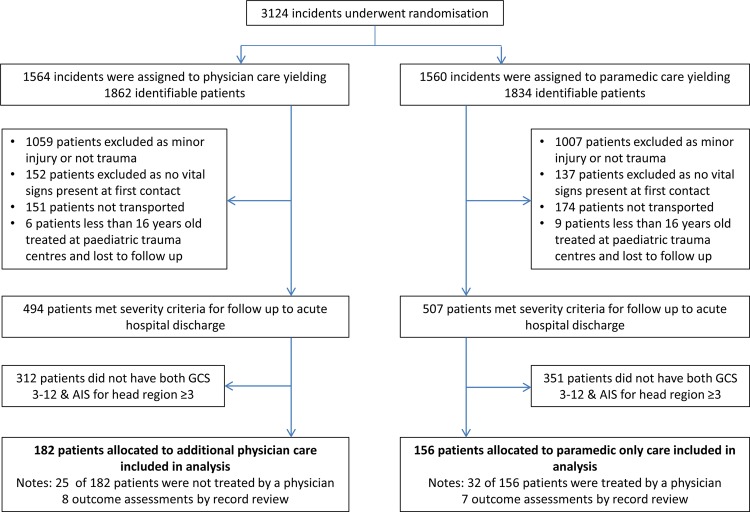
Methods: Participants in this prospective, randomised controlled trial were adult patients with blunt trauma with either a scene GCS score <9 (original definition), or GCS<13 and an Abbreviated Injury Scale score for the head region ≥3 (modified definition). Patients were randomised to either standard ground paramedic treatment or standard treatment plus a physician arriving by helicopter. Patients were evaluated by 30-day mortality and 6-month Glasgow Outcome Scale (GOS) scores. Due to high non-compliance rates, both intention-to-treat and as-treated analyses were preplanned.
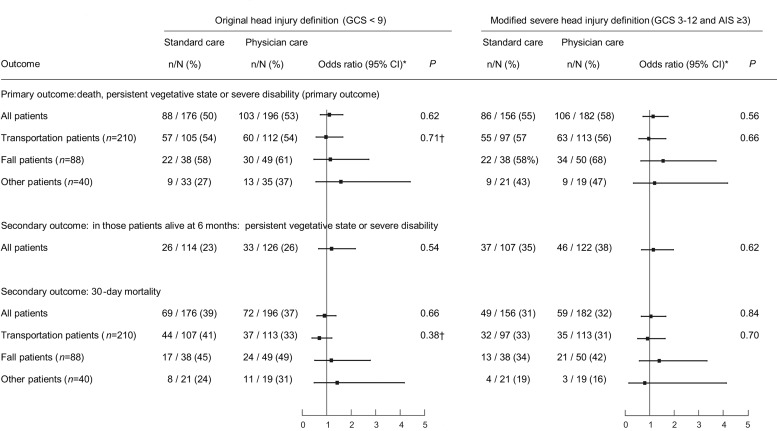
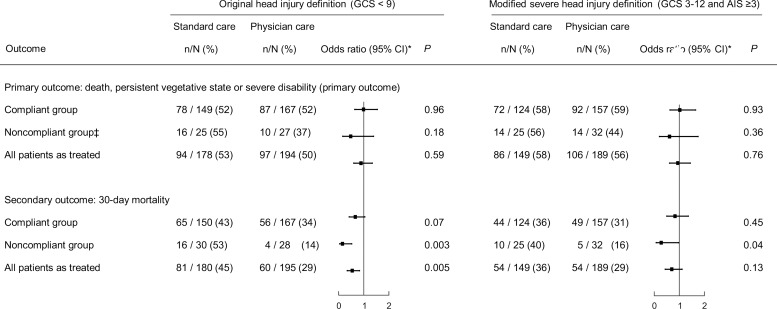
Results: 375 patients met the original definition, of which 197 was allocated to physician care. Differences in the 6-month GOS scores were not significant on intention-to-treat analysis (OR 1.11, 95% CI 0.74 to 1.66, p=0.62) nor was the 30-day mortality (OR 0.91, 95% CI 0.60 to 1.38, p=0.66). As-treated analysis showed a 16% reduction in 30-day mortality in those receiving additional physician care; 60/195 (29%) versus 81/180 (45%), p<0.01, Number needed to treat =6. 338 patients met the modified definition, of which 182 were allocated to physician care. The 6-month GOS scores were not significantly different on intention-to-treat analysis (OR 1.14, 95% CI 0.73 to 1.75, p=0.56) nor was the 30-day mortality (OR 1.05, 95% CI 0.66 to 1.66, p=0.84). As-treated analyses were also not significantly different.
Conclusions: This trial suggests a potential mortality reduction in patients with blunt trauma with GCS<9 receiving additional physician care (original definition only). Confirmatory studies which also address non-compliance issues are needed.
Trial registration number: NCT00112398.
Keywords: Trauma, head; comparitive system research; emergency ambulance systems, effectiveness; prehospital care, doctors in PHC; prehospital care, helicopter retrieval.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Garner AA, Fearnside M, Gebski V. The study protocol for the Head Injury Retrieval Trial (HIRT): a single centre randomised controlled trial of physician pre-hospital management of severe blunt head injury compared with management by paramedics. Scand J Trauma Resusc Emerg Med 2013;21:69 10.1186/1757-7241-21-69 - DOI - PMC - PubMed
-
- Early Management of Severe Trauma course content. Royal Australasian College of Surgeons 2013. http://www.surgeons.org/for-health-professionals/register-courses-events... (accessed 30 Dec 2013).
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous