

Rapid resolution of retinoschisis with acetazolamide
- PMID: 25796216
- PMCID: PMC4504776
- DOI: 10.1007/s10633-015-9496-8
Rapid resolution of retinoschisis with acetazolamide
Abstract
Purpose: To report the results of an acetazolamide (Diamox(®)) treatment regimen in a genetically confirmed case of X-linked juvenile retinoschisis (XLRS).
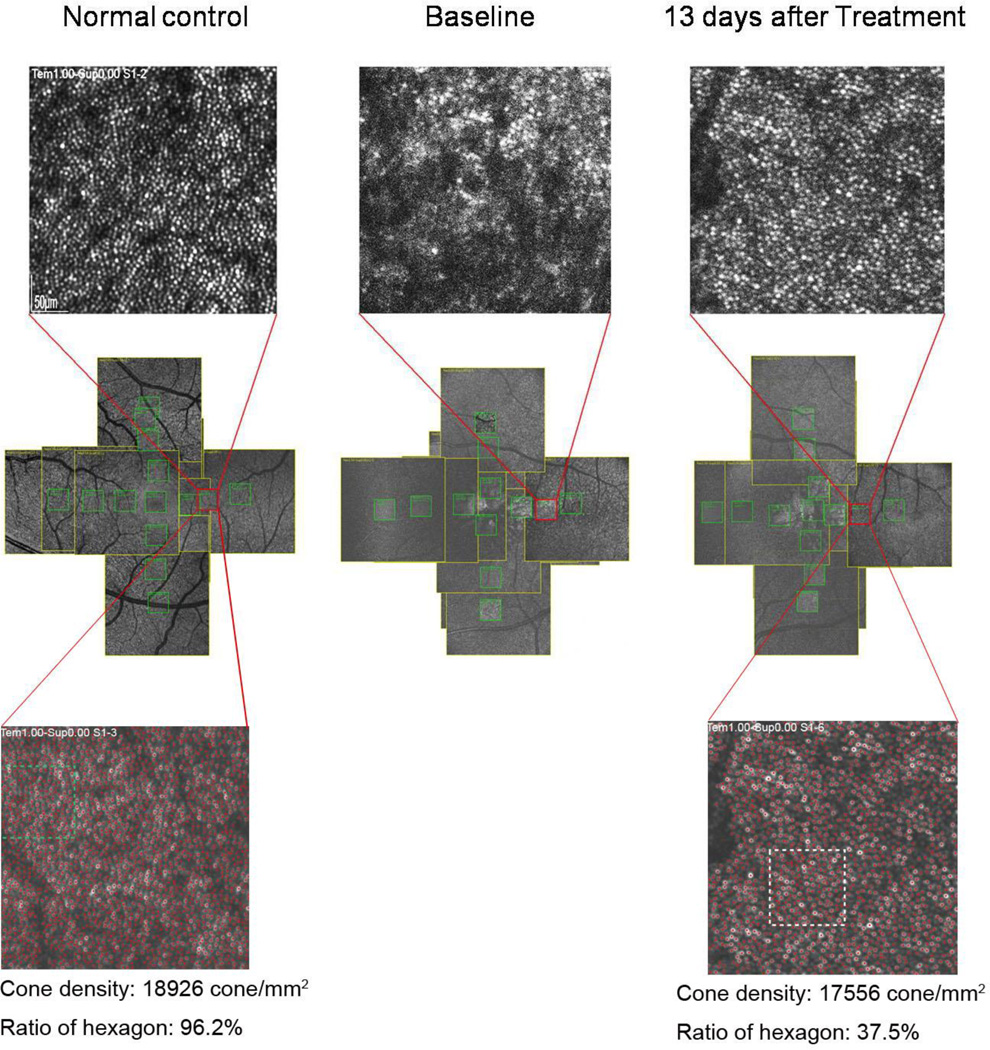
Methods: A patient with XLRS was prescribed acetazolamide (Diamox(®)) at a dose of 500 mg/day, then discontinued the treatment due to non-compliance for 4 days, and finally resumed the course of treatment. Best-corrected visual acuity, retinal structure, and function were monitored with autofluorescence, spectral domain-optical coherence tomography (SD-OCT), adaptive optics scanning laser ophthalmoscopy (AOSLO), and full-field electroretinogram (ERG). Full-field ERG was performed using DTL recording electrodes and Ganzfeld stimulation according to ISCEV standards.
Results: Serial monitoring of the cysts by SD-OCT revealed a strong association between the effects of acetazolamide administration and the size of the schisis. A reduction in foveal cyst size was significant in as rapid as 6 days after acetazolamide initiation. AOSLO data revealed that the resolution of cone cell images improves as the foveal schisis decreases in size.
Conclusions: Efficacy of acetazolamide in patients with XLRS can be apparent in as rapid as a week of therapy. AOSLO can be a good method to evaluate the cone cells after acetazolamide treatment in the early stages of XLRS.
Conflict of interest statement
Figures





References
-
- Tantri A, Vrabec TR, Cu-Unjieng A, Frost A, Annesley WH, Jr, Donoso LA. X-linked retinoschisis: a clinical and molecular genetic review. Surv Ophthalmol. 2004;49(2):214–230. - PubMed
-
- Gregori NZ, Berrocal AM, Gregori G, Murray TG, Knighton RW, Flynn HW, Jr, Dubovy S, Puliafito CA, Rosenfeld PJ. Macular spectral-domain optical coherence tomography in patients with X linked retinoschisis. Br J Ophthalmol. 2009;93(3):373–378. - PubMed
-
- Wu WW, Wong JP, Kast J, Molday RS. RS1, a discoidin domain-containing retinal cell adhesion protein associated with X-linked retinoschisis, exists as a novel disulfide-linked octamer. J Biol Chem. 2005;280(11):10721–10730. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
