

Left ventricular assist devices: a kidney's perspective
- PMID: 25796403
- PMCID: PMC4464048
- DOI: 10.1007/s10741-015-9481-z
Left ventricular assist devices: a kidney's perspective
Abstract
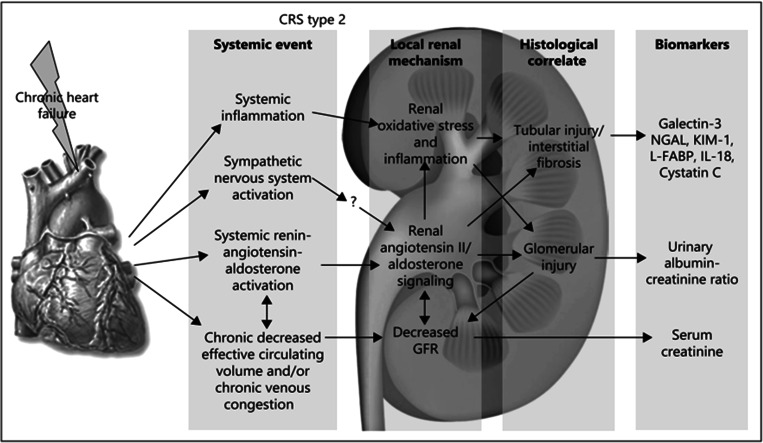
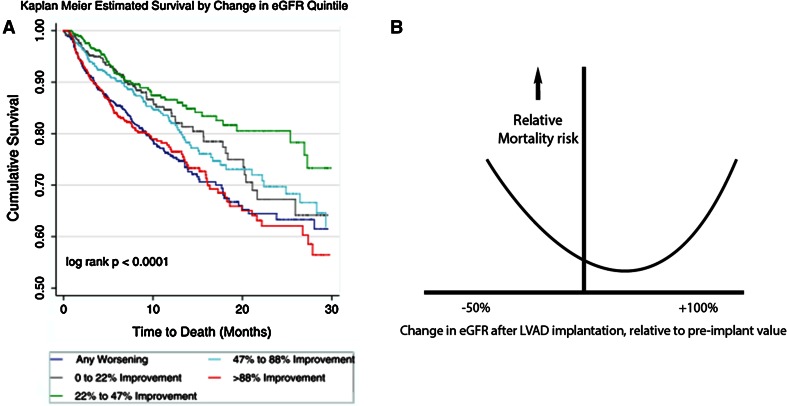
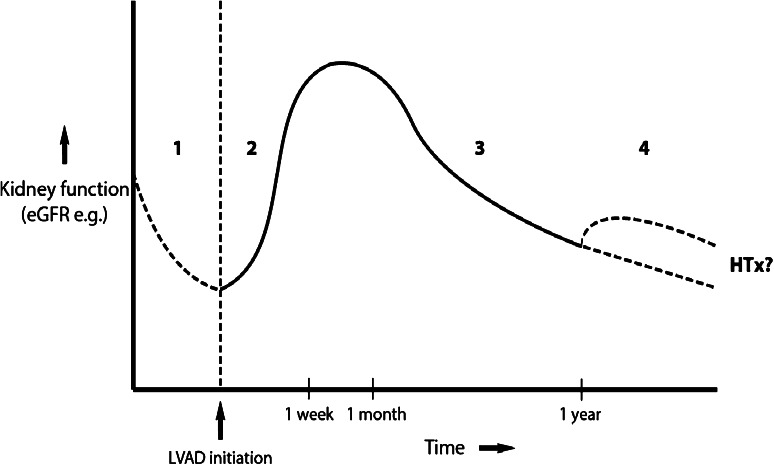
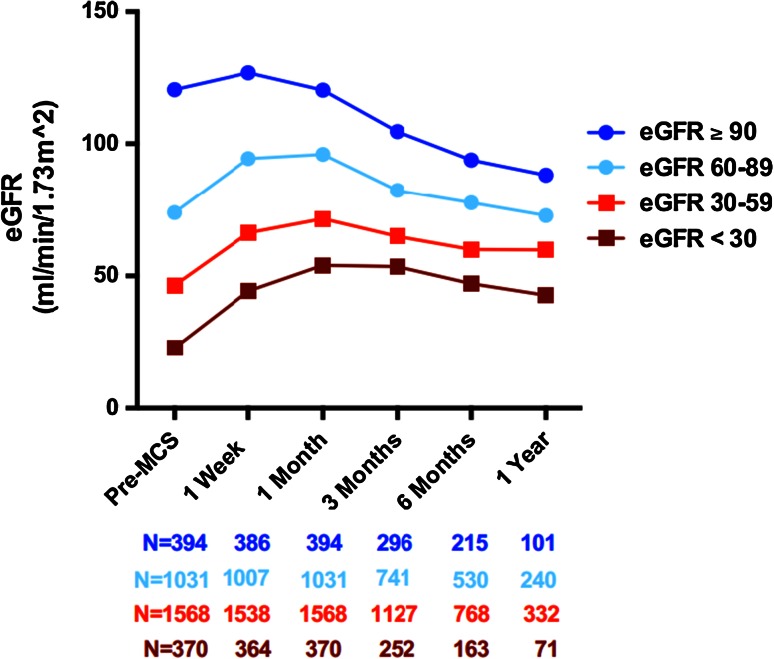
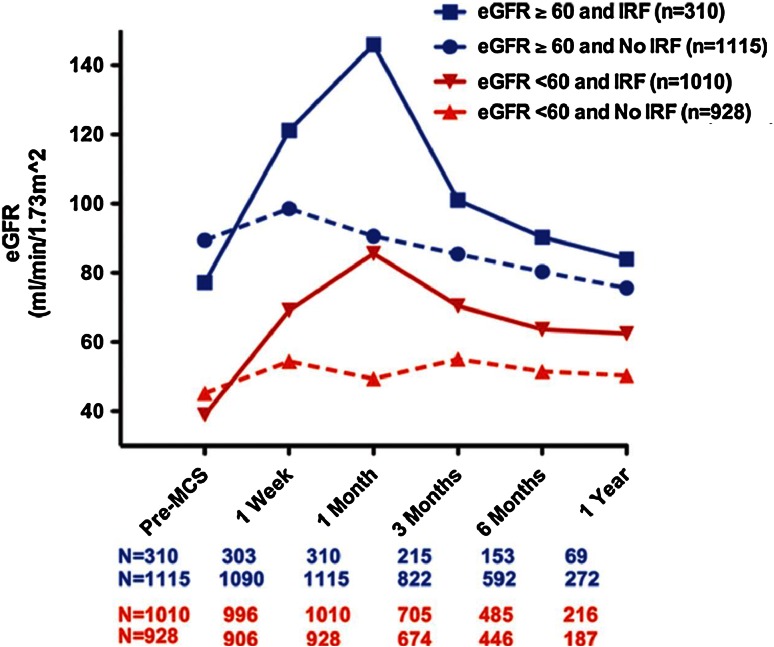
The left ventricular assist device (LVAD) has become an established treatment option for patients with refractory heart failure. Many of these patients experience chronic kidney disease (CKD) due to chronic cardiorenal syndrome type II, which is often alleviated quickly following LVAD implantation. Nevertheless, reversibility of CKD remains difficult to predict. Interestingly, initial recovery of GFR appears to be transient, being followed by gradual but significant late decline. Nevertheless, GFR often remains elevated compared to preimplant status. Larger GFR increases are followed by a proportionally larger late decline. Several explanations for this gradual decline in renal function after LVAD therapy have been proposed, yet a definitive answer remains elusive. Mortality predictors of LVAD implantation are the occurrence of either postimplantation acute kidney injury (AKI) or preimplant CKD. However, patient outcomes continue to improve as LVAD therapy becomes more widespread, and adverse events including AKI appear to decline. In light of a growing destination therapy population, it is important to understand the cumulative effects of long-term LVAD support on kidney function. Additional research and passage of time are required to further unravel the intricate relationships between the LVAD and the kidney.
Figures
Comment in
-
Letter to the Editor regarding the article "Left ventricular assist devices: a kidney's perspective".Heart Fail Rev. 2015 Nov;20(6):751-2. doi: 10.1007/s10741-015-9504-9. Heart Fail Rev. 2015. PMID: 26387095 No abstract available.
-
Absence of structural lesions in human renal arcuate arteries after LVAD implantation: response to a letter regarding "left ventricular assist devices: a kidney's perspective".Heart Fail Rev. 2015 Nov;20(6):753-4. doi: 10.1007/s10741-015-9507-6. Heart Fail Rev. 2015. PMID: 26395012 No abstract available.
References
-
- Seferovic PM, Stoerk S, Filippatos G, et al. Organization of heart failure management in European Society of Cardiology member countries: survey of the Heart Failure Association of the European Society of Cardiology in collaboration with the Heart Failure National Societies/Working Groups. Eur J Heart Fail. 2013;15(9):947–959. - PubMed
-
- Ammirati E, Oliva F, Cannata A, et al. Current indications for heart transplantation and left ventricular assist device: a practical point of view. Eur J Intern Med. 2014;25(5):422–429. - PubMed
-
- Jessup M, Brozena S. Heart failure. N Engl J Med. 2003;348(20):2007–2018. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
