

Preterm cord blood CD4⁺ T cells exhibit increased IL-6 production in chorioamnionitis and decreased CD4⁺ T cells in bronchopulmonary dysplasia
- PMID: 25797206
- PMCID: PMC4507273
- DOI: 10.1016/j.humimm.2015.03.007
Preterm cord blood CD4⁺ T cells exhibit increased IL-6 production in chorioamnionitis and decreased CD4⁺ T cells in bronchopulmonary dysplasia
Abstract
Background: Chorioamnionitis (CA) is associated with premature delivery and bronchopulmonary dysplasia (BPD). We hypothesize that preterm infants exposed to CA have reduced suppressive regulatory T cells (Treg) and increased non-regulatory T cell pro-inflammatory cytokines, increasing risk for BPD.
Objective: To evaluate cord blood CD4(+) T cell regulatory phenotype and pro-inflammatory cytokine production in CA and BPD groups.
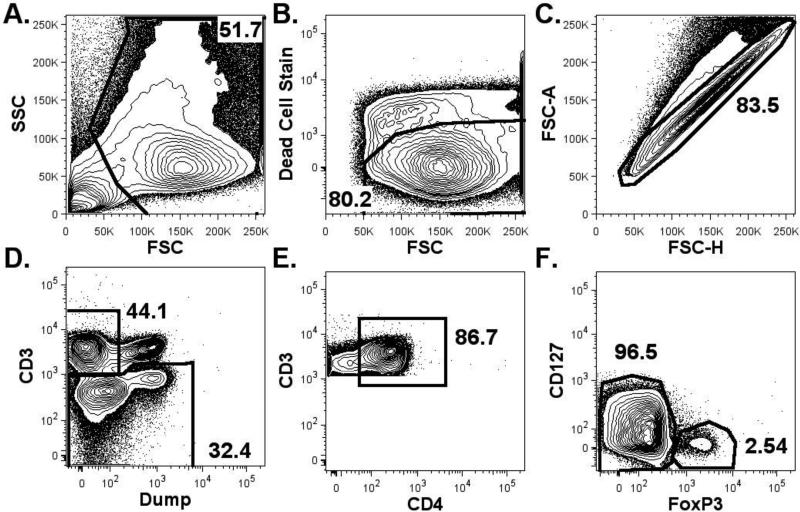
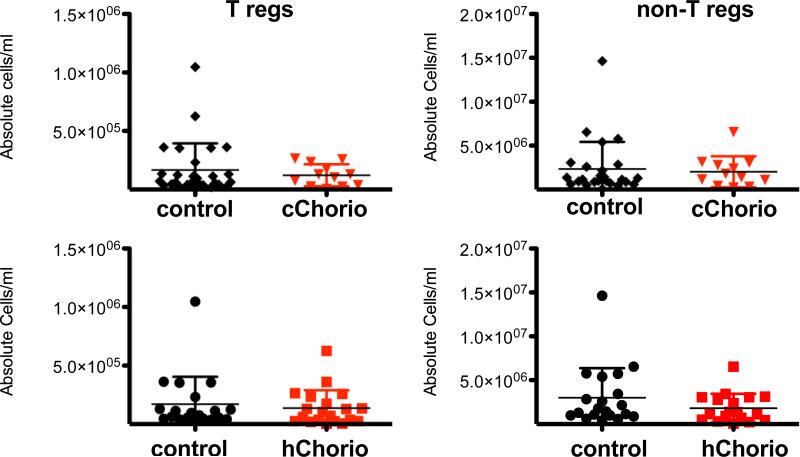
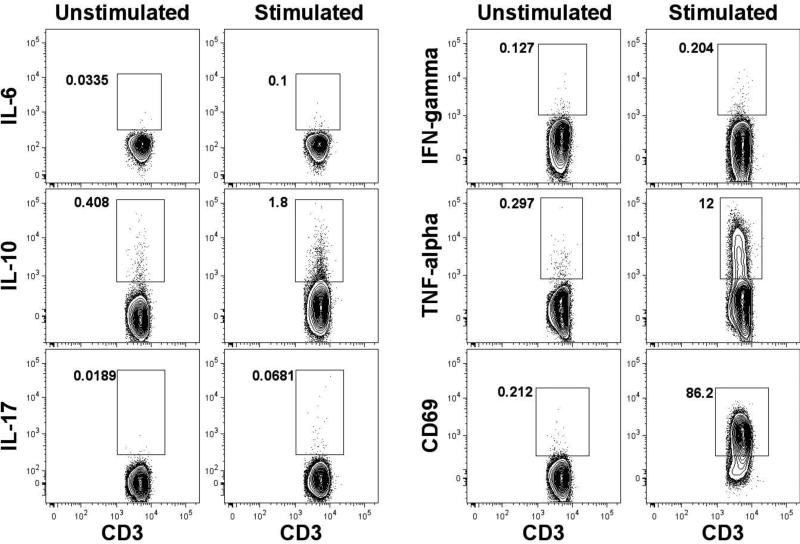
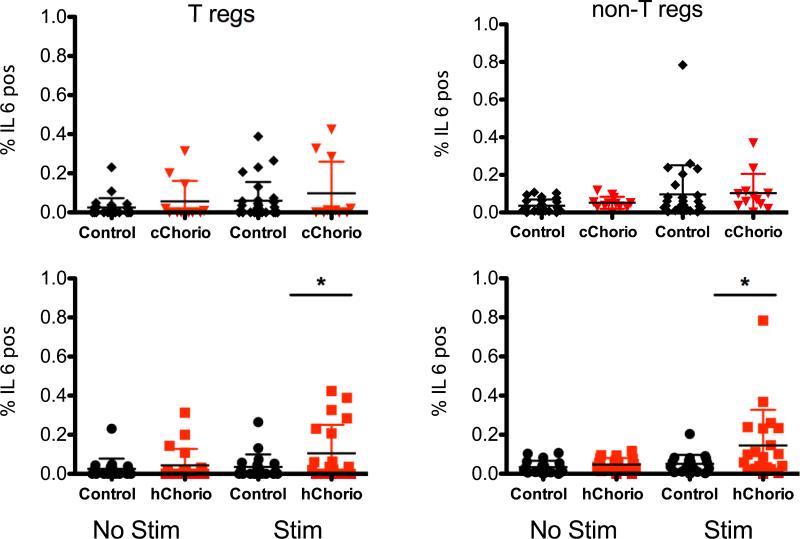
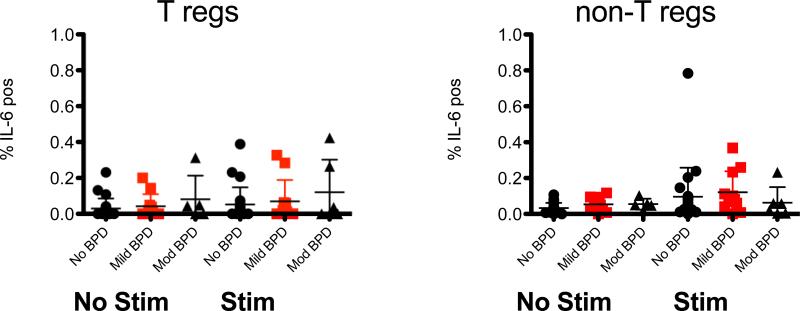
Study design: Cord blood mononuclear cells from infants (GA ⩽32 weeks), with or without placental histological evidence of CA (hChorio), were analyzed by flow cytometry. Clinical information was collected by retrospective chart review. Numbers of putative Treg (CD4(+)FoxP3(+)CD25(+)CD127Dim), CD4(+) non-Tregs, and CD4(+) T cell intracellular cytokine content following in vitro stimulation were compared with CA status and oxygen requirement at 36weeks postmenstrual age.
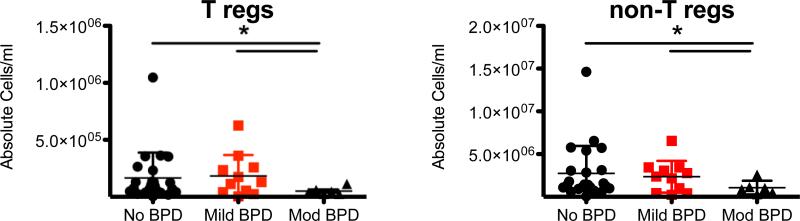
Result: Absolute Treg numbers were not different in CA and non-CA exposed samples. However, the infants who developed BPD had a significant decrease in Treg and non-regulatory T cell numbers. Greater IL-6 production was observed in hCA group.
Conclusion: A pro-inflammatory CD4(+) T cell status is noted in CA and BPD but the later disease is also associated with decrease in Tregs, suggesting that the development of BPD is marked by distinct inflammatory changes from those of CA exposed infants.
Keywords: Bronchopulmonary dysplasia; CD4(+) T cells; Chorioamnionitis; Cord blood mononuclear cell; IL-6.
Copyright © 2015 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Fanaroff AA, et al. Trends in neonatal morbidity and mortality for very low birthweight infants. Am J Obstet Gynecol. 2007;196(2):147, e1–8. - PubMed
-
- Wong PM, et al. Emphysema in young adult survivors of moderate-to-severe bronchopulmonary dysplasia. Eur Respir J. 2008;32(2):321–8. - PubMed
-
- Baraldi E, et al. Pulmonary function until two years of life in infants with bronchopulmonary dysplasia. Am J Respir Crit Care Med. 1997;155(1):149–55. - PubMed
-
- Kennedy JD, et al. Effects of birthweight and oxygen supplementation on lung function in late childhood in children of very low birth weight. Pediatr Pulmonol. 2000;30(1):32–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
