

Superior turbinectomy: role for a two-surgeon technique in endoscopic endonasal transsphenoidal surgery--technical note
- PMID: 25797783
- PMCID: PMC4628182
- DOI: 10.2176/nmc.tn.2014-0159
Superior turbinectomy: role for a two-surgeon technique in endoscopic endonasal transsphenoidal surgery--technical note
Abstract
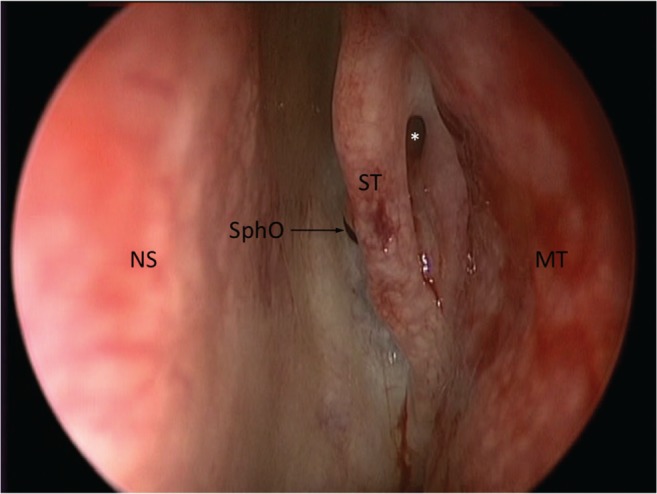
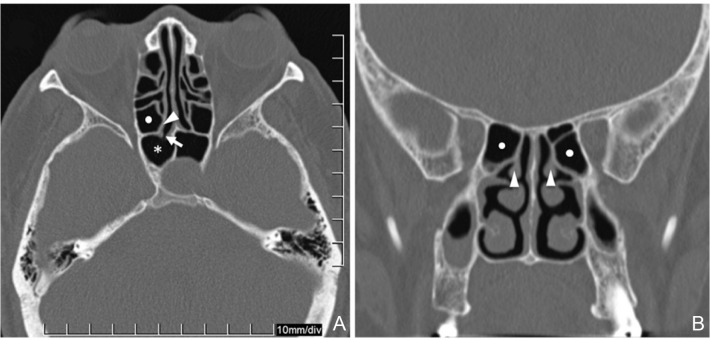
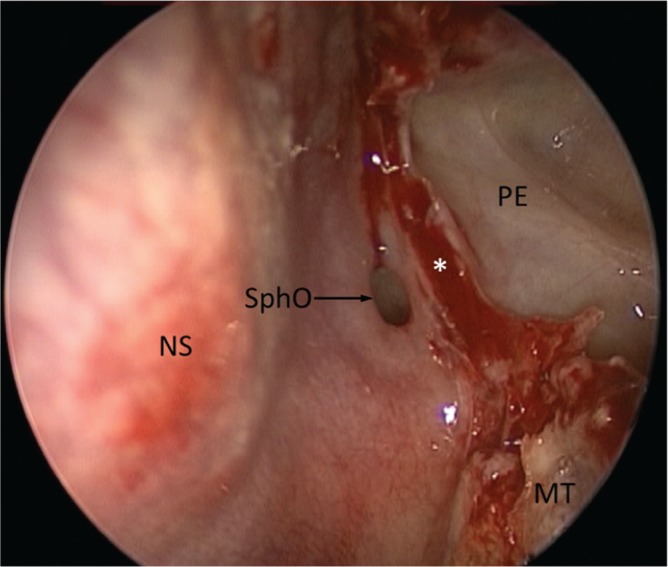
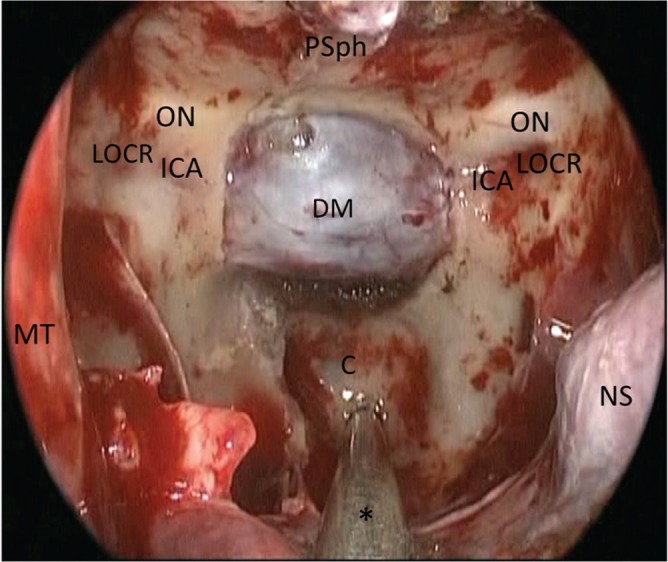
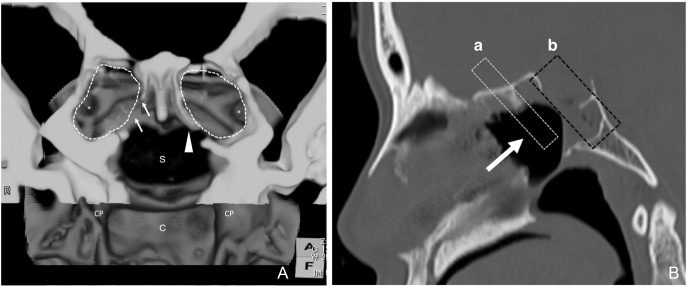
We describe a practical technique of superior turbinectomy followed by posterior ethmoidectomy as a less invasive procedure for two-surgeon technique on endoscopic endonasal transsphenoidal surgery. After identification of the superior turbinate and the sphenoid ostium, the inferior third portion of the superior turbinate was coagulated and resected. This partial superior turbinectomy procedure exposed the posterior ethmoidal sinus. Resection of the bony walls between the sphenoid and posterior ethmoid sinuses provided more lateral and superior exposure of the sphenoid sinus. This technique was performed in 56 patients with midline skull base lesions, including 49 pituitary adenomas and 7 other lesions. Meticulous manipulation of instruments was performed in all cases without surgical complications such as permanent hyposmia/anosmia or nasal bleeding. Our findings suggested that the partial superior turbinectomy followed by retrograde posterior ethmoidectomy is a simple and safe technique providing a sufficient surgical corridor for two-surgeon technique to approaching midline skull base regions, mainly involving pituitary adenomas.
Conflict of interest statement
All of authors have nothing to be disclosed as conflicts of interest (COI). Yasunori Fujimoto, Akatsuki Wakayama, and Toshiki Yoshimine are members of the Japan Neurosurgical Society, and their COI status have been disclosed to the COI committee of the society. Henrique F. Ramos, Pedro P. Mariani, Fabrizio R. Romano, Arthur Cukiert, and Edson Bor-Seng-Shu, are not members of the society, and they have nothing to be disclosed as COI.
Figures
References
-
- Orlandi RR, Lanza DC, Bolger WE, Clerico DM, Kennedy DW: The forgotten turbinate: the role of the superior turbinate in endoscopic sinus surgery. Am J Rhinol 13: 251– 259, 1999. - PubMed
-
- Eweiss AZ, Ibrahim AA, Khalil HS: The safe gate to the posterior paranasal sinuses: reassessing the role of the superior turbinate. Eur Arch Otorhinolaryngol 269: 1451– 1456, 2012. - PubMed
-
- Bolger WE, Keyes AS, Lanza DC: Use of the superior meatus and superior turbinate in the endoscopic approach to the sphenoid sinus. Otolaryngol Head Neck Surg 120: 308– 313, 1999. - PubMed
-
- Har-El G, Swanson RM: The superior turbinectomy approach to isolated sphenoid sinus disease and to the sella turcica. Am J Rhinol 15: 149– 156, 2001. - PubMed
-
- Millar DA, Orlandi RR: The sphenoid sinus natural ostium is consistently medial to the superior turbinate. Am J Rhinol 20: 180– 181, 2006. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources