

Surgical Methods for the Treatment of Uterine Fibroids - Risk of Uterine Sarcoma and Problems of Morcellation: Position Paper of the DGGG
- PMID: 25797958
- PMCID: PMC4361164
- DOI: 10.1055/s-0035-1545684
Surgical Methods for the Treatment of Uterine Fibroids - Risk of Uterine Sarcoma and Problems of Morcellation: Position Paper of the DGGG
Abstract
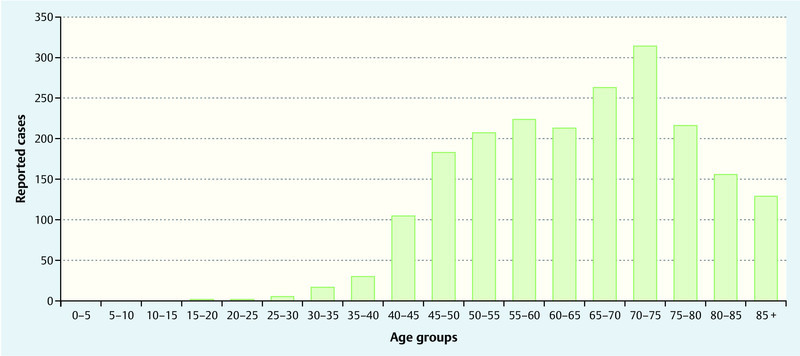
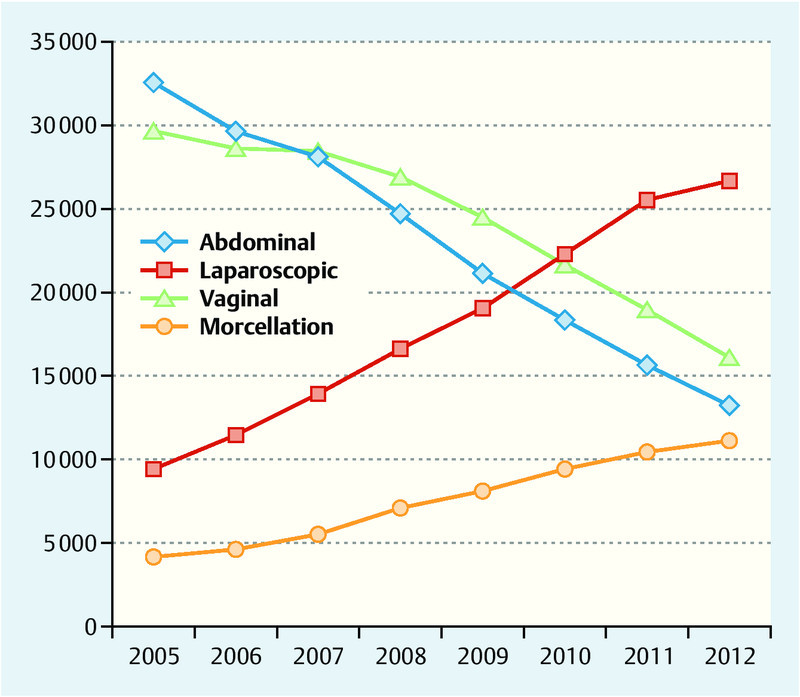
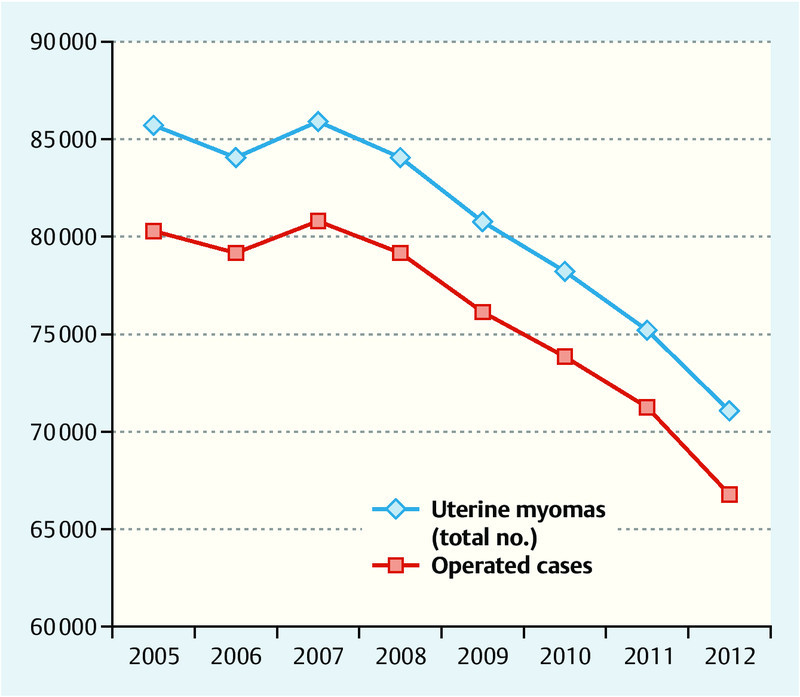
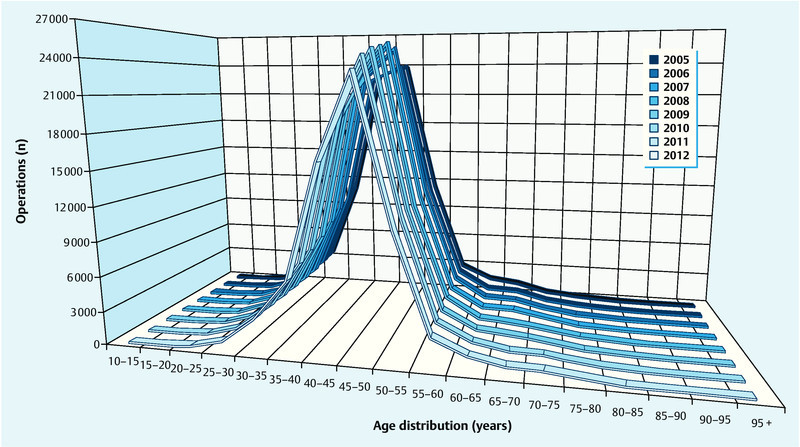
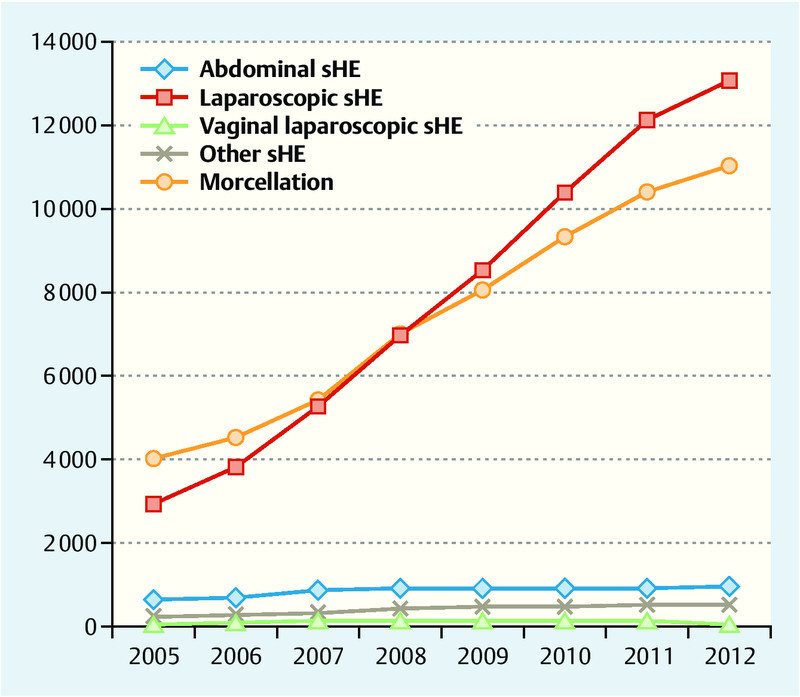
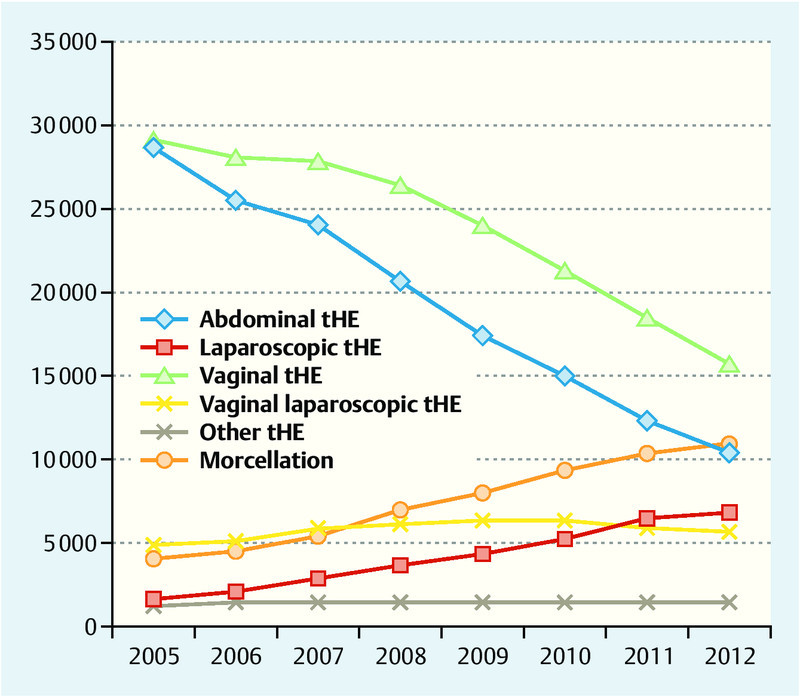
The appropriate surgical technique to treat patients with uterine fibroids is still a matter of debate as is the potential risk of incorrect treatment if histological examination detects a uterine sarcoma instead of uterine fibroids. The published epidemiology for uterine sarcoma is set against the incidence of accidental findings during surgery for uterine fibroids. International comments on this topic are discussed and are incorporated into the assessment by the German Society for Gynecology and Obstetrics (DGGG). The ICD-O-3 version of 2003 was used for the anatomical and topographical coding of uterine sarcomas, and the "Operations- und Prozedurenschlüssel" (OPS) 2014, the German standard for process codes and interventions, was used to determine surgical extirpation methods. Categorical qualifiers were defined to analyze the data provided by the Robert Koch Institute (RKI), the German Federal Bureau of Statistics (DESTATIS; Hospital and Causes of Death Statistics), the population-based Cancer Register of Bavaria. A systematic search was done of the MEDLINE database and the Cochrane collaboration, covering the period from 1966 until November 2014. The incidence of uterine sarcoma and uterine fibroids in uterine surgery was compared to the literature and with the different registries. The incidence of uterine sarcoma in 2010, standardized for age, was 1.53 for Bavaria, or 1.30 for every 100 000 women, respectively, averaged for the years 2002-2011, and 1.30 for every 100 000 women in Germany. The mean incidence collated from various surveys was 2.02 for every 100 000 women (0.35-7.02; standard deviation 2.01). The numbers of inpatient surgical procedures such as myoma enucleation, morcellation, hysterectomy or cervical stump removal to treat the indication "uterine myoma" have steadily declined in Germany across all age groups (an absolute decrease of 17 % in 2012 compared to 2007). There has been a shift in the preferred method of surgical access from an abdominal/vaginal approach to endoscopic or endoscopically assisted procedures to treat uterine fibroids, with the use of morcellation increasing by almost 11 000 coded procedures in 2012. Based on international statements (AAGL, ACOG, ESGE, FDA, SGO) on the risk of uterine sarcoma as an coincidental finding during uterine fibroid surgery and the associated risk of a deterioration of prognosis (in the case of morcellation procedures), this overview presents the opinion of the DGGG in the form of four Statements, five Recommendation and four Demands.
In der Behandlung der Patientin mit Uterus myomatosus gibt es Diskussionen über die Art der Operationstechnik und das damit verbundene Risiko der eventuellen falschen Behandlung, wenn sich in der histologischen Aufarbeitung keine Uterusmyome, sondern ein Uterussarkom herausstellt. Die publizierte Epidemiologie von Uterussarkomen wird hier ins Verhältnis zu Zufallsbefunden bei Operationen zur Behandlung von Uterusmyomen gesetzt. Die internationalen Stellungnahmen zu diesem Thema werden diskutiert, um eine Bewertung seitens der Deutschen Gesellschaft für Gynäkologie und Geburtshilfe (DGGG) abzugeben. Zur anatomischen und topografischen Codierung der Uterussarkome wurde der ICD-O-3 in der Ausgabe von 2003 und für die Operations- und Prozedurenschlüssel der exstirpierenden Verfahren der OPS 2014 benutzt. Um die übermittelten Daten des Robert Koch-Instituts (RKI), des Statistischen Bundesamts (DESTATIS; Abteilung Krankenhausstatistik und Todesursachenstatistik), des bevölkerungsbezogenen Krebsregisters Bayern auswerten zu können, wurden eindeutige Abfragekriterien definiert. Zusätzlich wurde eine systematische Literaturrecherche in MEDLINE von 1966 bis November 2014 und bei der Cochrane Collaboration durchgeführt. Die Inzidenz von Uterussarkomen und Uterusmyomen bei Operationen der Gebärmutter wurden in den verschiedenen Registern und in der Literatur verglichen. Die altersstandardisierte Inzidenz im Jahr 2010 für Uterussarkome war für Bayern 1,53, respektive 1,30 auf 100 000 Frauen gemittelt über die Jahre 2002–2011, in Deutschland bei 1,30 auf 100 000 Frauen. Die mittlere Inzidenz aus verschiedenen Erhebungen beträgt 2,02 auf 100 000 Frauen (0,35–7,02; Standardabweichung 2,01). Stationär durchgeführte Operationen wie Myomenukleation, Morcellation, Hysterektomie oder Zervixstumpfresektion sind bei der Indikation Uterusmyom in Deutschland gleichbleibend über alle Altersgruppen hinweg zurückgegangen (absoluter Rückgang von 17 % im Jahr 2012 zum Jahr 2007). Es zeigt sich eine Verschiebung des operativen Zugangswegs von abdominal/vaginal zu endoskopisch bzw. endoskopisch assistierten zur Behandlung von Uterusmyomen mit einer ansteigenden Benutzung der Morcellation von fast 11 000 codierten Prozeduren im Jahr 2012. Nach den Veröffentlichungen von internationalen Stellungnahmen (AAGL, ACOG, ESGE, FDA, SGO) zum Risiko Uterussarkom als Zufallsbefund im Rahmen einer Myomoperation und dem damit verbundenen Risiko einer Prognoseverschlechterung (im Falle einer Morcellation) wird in dieser Übersichtsarbeit die DGGG-Stellungnahme in Form von 4 Statements, 5 Empfehlungen und 4 Forderungen dargestellt.
Keywords: epidemiology; hysterectomy; morcellation; myomectomy; uterine fibroid; uterine sarcoma.
Conflict of interest statement
Figures


Similar articles
-
The management of uterine leiomyomas.J Obstet Gynaecol Can. 2015 Feb;37(2):157-178. doi: 10.1016/S1701-2163(15)30338-8. J Obstet Gynaecol Can. 2015. PMID: 25767949
-
Can the risks associated with uterine sarcoma morcellation really be prevented? Overview of the role of uterine morcellation in 2018.J Gynecol Obstet Hum Reprod. 2018 Oct;47(8):341-349. doi: 10.1016/j.jogoh.2018.05.015. Epub 2018 Jun 4. J Gynecol Obstet Hum Reprod. 2018. PMID: 29879489 Review.
-
A Retrospective Analysis of the Impact of Myomectomy on Survival in Uterine Sarcoma.PLoS One. 2016 Feb 1;11(2):e0148050. doi: 10.1371/journal.pone.0148050. eCollection 2016. PLoS One. 2016. PMID: 26828206 Free PMC article.
-
Incidence of Tissue Morcellation During Surgery for Uterine Sarcoma at a Canadian Academic Centre.J Obstet Gynaecol Can. 2015 May;37(5):421-425. doi: 10.1016/S1701-2163(15)30256-5. J Obstet Gynaecol Can. 2015. PMID: 26168102
-
Laparoscopic power morcellation of presumed fibroids.Minerva Ginecol. 2016 Jun;68(3):352-63. Epub 2016 Jan 22. Minerva Ginecol. 2016. PMID: 26799759 Review.
Cited by
-
Diagnosis and treatment of submucous myoma of the uterus with interventional ultrasound.Oncol Lett. 2018 May;15(5):6189-6194. doi: 10.3892/ol.2018.8122. Epub 2018 Feb 27. Oncol Lett. 2018. PMID: 29616100 Free PMC article.
-
Arterial hypertension as an inaugural sign of myomatous uterus.BMJ Case Rep. 2021 Jul 20;14(7):e243270. doi: 10.1136/bcr-2021-243270. BMJ Case Rep. 2021. PMID: 34285027 Free PMC article.
-
Sarcoma of the Uterus. Guideline of the DGGG, OEGGG and SGGG (S2k-Level, AWMF Registry No. 015/074, April 2021).Geburtshilfe Frauenheilkd. 2022 Dec 1;82(12):1337-1367. doi: 10.1055/a-1897-5124. eCollection 2022 Dec. Geburtshilfe Frauenheilkd. 2022. PMID: 36467974 Free PMC article.
-
Sarcoma of the Uterus. Guideline of the DGGG (S2k-Level, AWMF Registry No. 015/074, August 2015).Geburtshilfe Frauenheilkd. 2015 Oct;75(10):1028-1042. doi: 10.1055/s-0035-1558120. Geburtshilfe Frauenheilkd. 2015. PMID: 26640293 Free PMC article.
-
Frequency of uterine sarcomas in patients admitted for uterine fibroid surgery.J Turk Ger Gynecol Assoc. 2017 Jun 1;18(2):62-66. doi: 10.4274/jtgga.2016.0248. Epub 2017 Feb 7. J Turk Ger Gynecol Assoc. 2017. PMID: 28400352 Free PMC article.
References
-
- U.S. Food and Drug Administration Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA safety communicationOnline:http://www.fda.gov/medicaldevices/safety/alertsandnotices/ucm393576.htmlast access: 15.07.2014
-
- Society of Gynecologic Oncology SGO position statement: morcellationOnline:https://www.sgo.org/newsroom/position-statements-2/morcellation/last access:15.07.2014
-
- Society of Gynecologic Oncology Statement of the SGO to the FDAʼs Obstetrics and Gynecology Medical Devices Advisory Committee concerning safety of laparoscopic power morcellationOnline:https://www.sgo.org/wp-content/uploads/2014/04/SGO-Testimony-to-FDA-on-P...last access: 15.07.2014
-
- U.S. Food and Drug Administration Updated laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA safety communicationOnline:http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm424443.htmlast access: 24.11.2014
-
- AAGL Advancing Minimally Invasive Gynecology Worldwide . AAGL practice report: Morcellation during uterine tissue extraction. J Minim Invasive Gynecol. 2014;21:517–530. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources