

Canadian Public Health Laboratory Network laboratory guidelines for congenital syphilis and syphilis screening in pregnant women in Canada
- PMID: 25798162
- PMCID: PMC4353984
- DOI: 10.1155/2015/589085
Canadian Public Health Laboratory Network laboratory guidelines for congenital syphilis and syphilis screening in pregnant women in Canada
Abstract
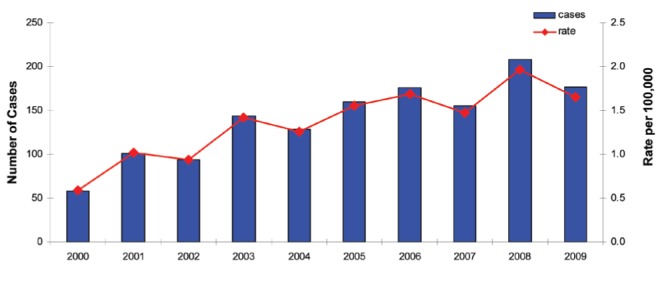
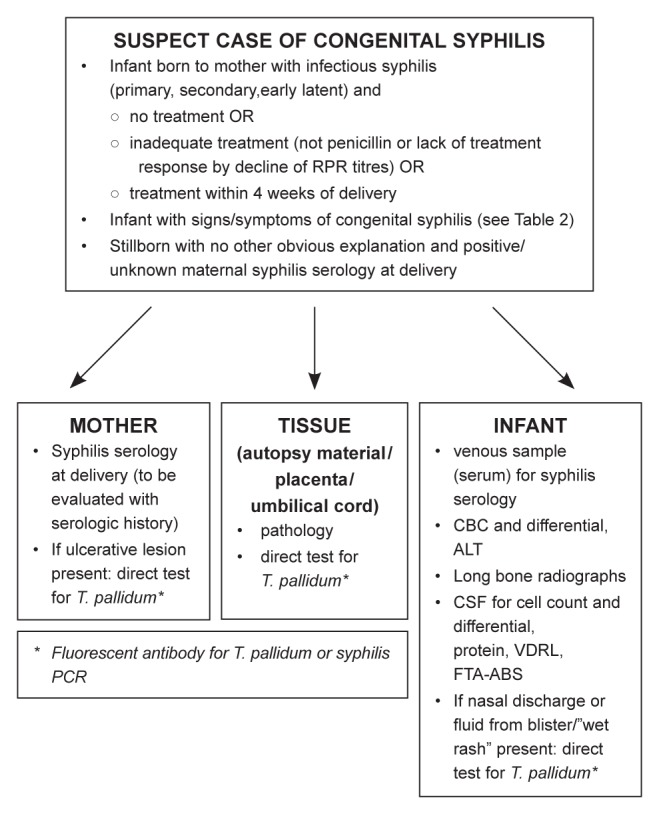
Despite universal access to screening for syphilis in all pregnant women in Canada, cases of congenital syphilis have been reported in recent years in areas experiencing a resurgence of infectious syphilis in heterosexual partnerships. Antenatal screening in the first trimester continues to be important and should be repeated at 28 to 32 weeks and again at delivery in women at high risk of acquiring syphilis. The diagnosis of congenital syphilis is complex and is based on a combination of maternal history and clinical and laboratory criteria in both mother and infant. Serologic tests for syphilis remain important in the diagnosis of congenital syphilis and are complicated by the passive transfer of maternal antibodies which can affect the interpretation of reactive serologic tests in the infant. All infants born to mothers with reactive syphilis tests should have nontreponemal tests (NTT) and treponemal tests (TT) performed in parallel with the mother's tests. A fourfold or higher titre in the NTT in the infant at delivery is strongly suggestive of congenital infection but the absence of a fourfold or greater NTT titre does not exclude congenital infection. IgM tests for syphilis are not currently available in Canada and are not recommended due to poor performance. Other evaluation in the newborn infant may include long bone radiographs and cerebrospinal fluid tests but all suspect cases should be managed in conjunction with sexually transmitted infection and/or pediatric experts.
Même si toutes les femmes du Canada ont accès au test de dépistage de la syphilis, des cas de syphilis congénitale ont été déclarés ces dernières années dans des régions où l’on constate une résurgence de la syphilis infectieuse chez des partenaires hétérosexuels. Il est toujours important de procéder à un dépistage anténatal pendant le premier trimestre, de le reprendre entre 28 et 32 semaines de grossesse, puis à l’accouchement chez les femmes très vulnérables à la syphilis. Le diagnostic de syphilis congénitale est complexe. Il repose sur l’histoire de la mère ainsi que sur des critères cliniques et des critères de laboratoire à la fois chez la mère et le nourrisson. Les tests sérologiques de la syphilis s’imposent toujours pour diagnostiquer la syphilis congénitale, mais ils sont compliqués par le transfert passif des anticorps maternels qui peut nuire à l’interprétation des résultats réactifs chez le nourrisson. Tous les nourrissons nés d’une mère dont les tests de syphilis sont réactifs devraient subir des tests non tréponomiques (TNT) et des tests tréponomiques (TT) conjointement aux tests de la mère. Un titrage du TNT au moins quatre fois plus élevé que la normale chez le nourrisson à l’accouchement est fortement évocateur d’une infection congénitale, mais l’absence d’un tel résultat n’en exclut pas la possibilité. Les tests d’IgM pour déceler la syphilis ne sont pas offerts au Canada. Ils ne sont pas recommandés en raison de leurs piètres résultats. Parmi les autres évaluations du nouveau-né, soulignons les radiographies des os longs et les tests du liquide céphalorachidien, mais il faut prendre en charge tous les cas présumés conjointement avec des pédiatres ou des spécialistes des infections transmises sexuellement.
Keywords: Canada; Congenital; Management; Pregnancy; Screening; Syphilis.
Figures
Similar articles
-
Early congenital syphilis: missed opportunities in a mother owing to many problems during pregnancy - a case report.Paediatr Int Child Health. 2022 May;42(2):89-94. doi: 10.1080/20469047.2022.2044676. Epub 2022 Apr 10. Paediatr Int Child Health. 2022. PMID: 35400316
-
Outcome of maternal syphilis at Rajavithi Hospital on offsprings.J Med Assoc Thai. 2005 Nov;88(11):1519-25. J Med Assoc Thai. 2005. PMID: 16471096
-
Syphilis in pregnant women in Zambia.Br J Vener Dis. 1982 Dec;58(6):355-8. doi: 10.1136/sti.58.6.355. Br J Vener Dis. 1982. PMID: 6756542 Free PMC article.
-
Recent trends in the serologic diagnosis of syphilis.Clin Vaccine Immunol. 2015 Feb;22(2):137-47. doi: 10.1128/CVI.00681-14. Epub 2014 Nov 26. Clin Vaccine Immunol. 2015. PMID: 25428245 Free PMC article. Review.
-
[Recent Advances in Laboratory Diagnosis of Syphilis].Mikrobiyol Bul. 2023 Jan;57(1):141-155. doi: 10.5578/mb.20239912. Mikrobiyol Bul. 2023. PMID: 36636853 Review. Turkish.
Cited by
-
[Sensitivity and specificity of epidemiological criteria for the case definition of congenital syphilis in a retrospective cohort in BrazilSensibilidad y especificidad de los criterios epidemiológicos para la definición de los casos de sífilis congénita en una cohorte retrospectiva en Brasil].Rev Panam Salud Publica. 2024 Dec 4;48:e133. doi: 10.26633/RPSP.2024.133. eCollection 2024. Rev Panam Salud Publica. 2024. PMID: 39635917 Free PMC article. Portuguese.
-
Syphilis in Ottawa: An evolving epidemic.Can Commun Dis Rep. 2022 Feb 24;48(2-3):76-82. doi: 10.14745/ccdr.v48i23a04. eCollection 2022 Feb 24. Can Commun Dis Rep. 2022. PMID: 35342370 Free PMC article.
-
Current Perspectives on Prevention of Mother-to-Child Transmission of Syphilis.Cureus. 2016 Mar 9;8(3):e525. doi: 10.7759/cureus.525. Cureus. 2016. PMID: 27081586 Free PMC article. Review.
-
Rising congenital syphilis rates in Canada, 1993-2022.Front Public Health. 2025 Jan 17;12:1522671. doi: 10.3389/fpubh.2024.1522671. eCollection 2024. Front Public Health. 2025. PMID: 39897185 Free PMC article.
-
Characteristics of polymerase chain reaction-positive syphilis cases in Manitoba, Canada, 2017 to 2020: Demographic analysis, specimen types, and Treponema pallidum gene targets.J Assoc Med Microbiol Infect Dis Can. 2022 Sep 27;7(3):170-180. doi: 10.3138/jammi-2022-0015. eCollection 2022 Sep. J Assoc Med Microbiol Infect Dis Can. 2022. PMID: 36337605 Free PMC article.
References
-
- Public Health Agency of Canada Report on Sexually Transmitted Infectious in Canada: 2011. < http://www.catie.ca/sites/default/files/64-02-14-1200-STI-Report-2011_EN...> (Accessed November 21, 2014)
-
- Public Health Agency of Canada Canadian Guidelines on Sexually Transmitted Infections, Syphilis chapter, 2010. < www.phac-aspc.gc.ca/std-mts/sti-its/pdf/510syphilis-eng.pdf> (Accessed December 8, 2010)
-
- Walker DG, Walker GJ. Forgotten but not gone: The continuing scourge of congenital syphilis. Lancet Infect Dis. 2002;2:432–6. - PubMed
-
- Centers for Disease Control and Prevention Sexually Transmitted Disease Treatment Guidelines, 2010. MMWR. 2010;59:RR-12. - PubMed
-
- Dorfman DH, Glaser JH. Congenital syphilis presenting in infants after the newborn period. N Engl J Med. 1990;323:1299–302. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
