

Safety and benefit of discontinuing statin therapy in the setting of advanced, life-limiting illness: a randomized clinical trial
- PMID: 25798575
- PMCID: PMC4618294
- DOI: 10.1001/jamainternmed.2015.0289
Safety and benefit of discontinuing statin therapy in the setting of advanced, life-limiting illness: a randomized clinical trial
Erratum in
-
Incorrect author name.JAMA Intern Med. 2015 May;175(5):869. doi: 10.1001/jamainternmed.2015.1600. JAMA Intern Med. 2015. PMID: 25938325 No abstract available.
-
Coding Error Resulting in Change in Secondary Outcome Scores.JAMA Intern Med. 2019 Jan 1;179(1):126-127. doi: 10.1001/jamainternmed.2018.7186. JAMA Intern Med. 2019. PMID: 30508017 Free PMC article. No abstract available.
Abstract
Importance: For patients with limited prognosis, some medication risks may outweigh the benefits, particularly when benefits take years to accrue; statins are one example. Data are lacking regarding the risks and benefits of discontinuing statin therapy for patients with limited life expectancy.
Objective: To evaluate the safety, clinical, and cost impact of discontinuing statin medications for patients in the palliative care setting.
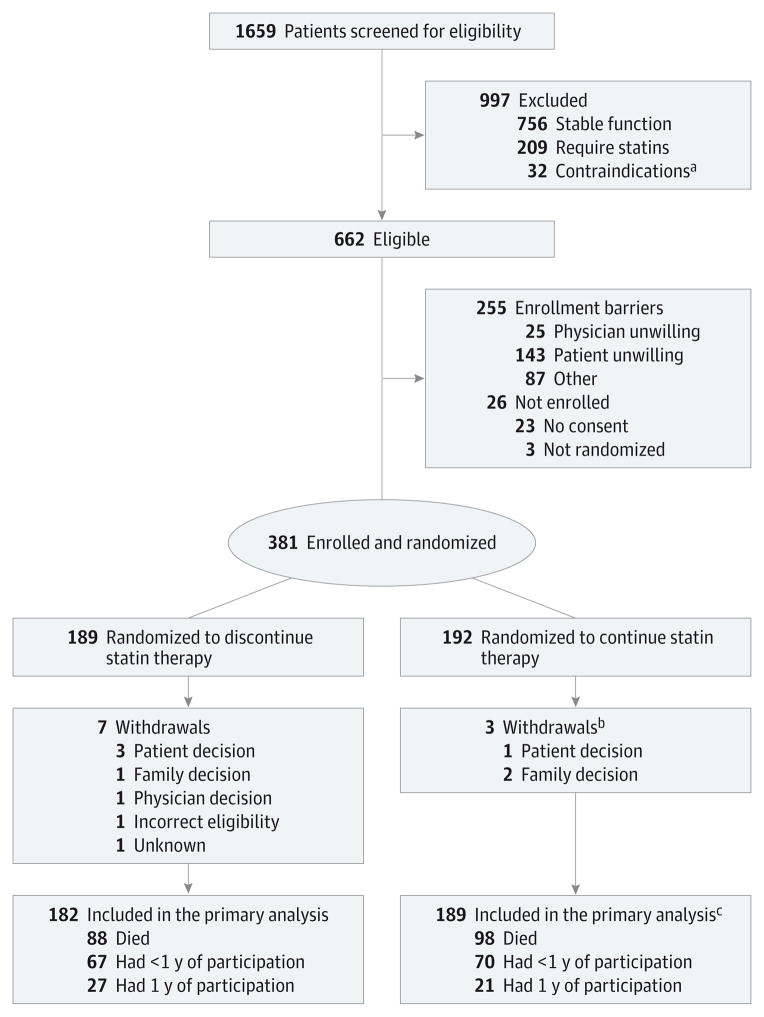
Design, setting, and participants: This was a multicenter, parallel-group, unblinded, pragmatic clinical trial. Eligibility included adults with an estimated life expectancy of between 1 month and 1 year, statin therapy for 3 months or more for primary or secondary prevention of cardiovascular disease, recent deterioration in functional status, and no recent active cardiovascular disease. Participants were randomized to either discontinue or continue statin therapy and were monitored monthly for up to 1 year. The study was conducted from June 3, 2011, to May 2, 2013. All analyses were performed using an intent-to-treat approach.
Interventions: Statin therapy was withdrawn from eligible patients who were randomized to the discontinuation group. Patients in the continuation group continued to receive statins.
Main outcomes and measures: Outcomes included death within 60 days (primary outcome), survival, cardiovascular events, performance status, quality of life (QOL), symptoms, number of nonstatin medications, and cost savings.
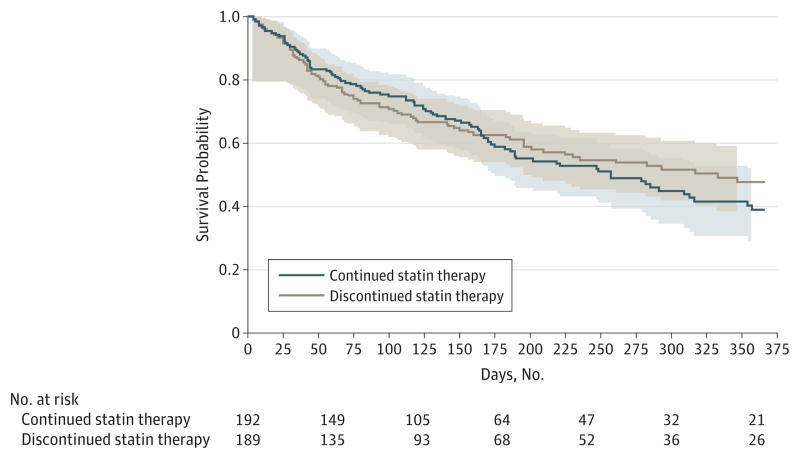
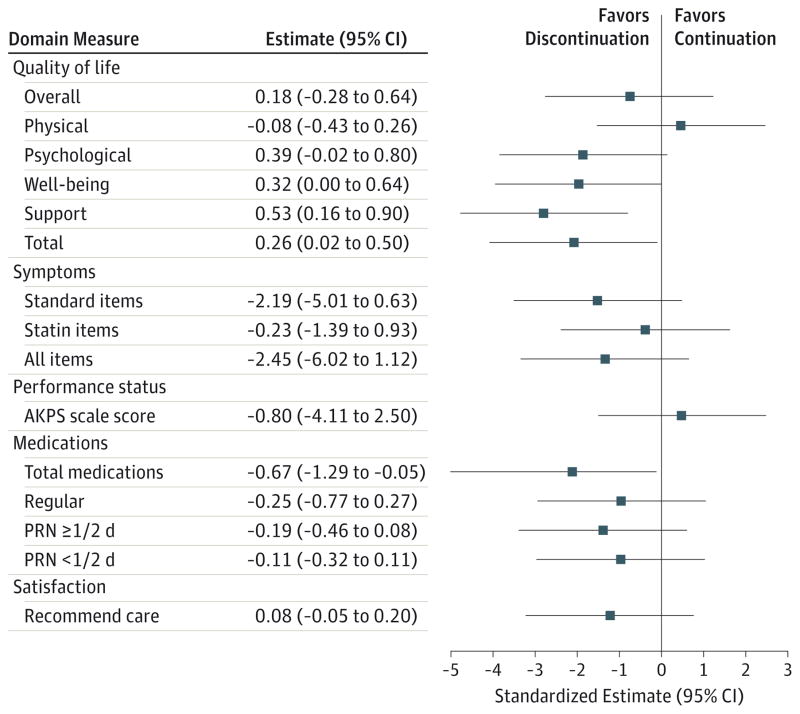
Results: A total of 381 patients were enrolled; 189 of these were randomized to discontinue statins, and 192 were randomized to continue therapy. Mean (SD) age was 74.1 (11.6) years, 22.0% of the participants were cognitively impaired, and 48.8% had cancer. The proportion of participants in the discontinuation vs continuation groups who died within 60 days was not significantly different (23.8% vs 20.3%; 90% CI, -3.5% to 10.5%; P=.36) and did not meet the noninferiority end point. Total QOL was better for the group discontinuing statin therapy (mean McGill QOL score, 7.11 vs 6.85; P=.04). Few participants experienced cardiovascular events (13 in the discontinuation group vs 11 in the continuation group). Mean cost savings were $3.37 per day and $716 per patient.
Conclusions and relevance: This pragmatic trial suggests that stopping statin medication therapy is safe and may be associated with benefits including improved QOL, use of fewer nonstatin medications, and a corresponding reduction in medication costs. Thoughtful patient-provider discussions regarding the uncertain benefit and potential decrement in QOL associated with statin continuation in this setting are warranted.
Trial registration: clinicaltrials.gov Identifier: NCT01415934.
Conflict of interest statement
Figures
Comment in
-
Evidence-based deprescribing of statins in patients with advanced illness.JAMA Intern Med. 2015 May;175(5):701-2. doi: 10.1001/jamainternmed.2015.0328. JAMA Intern Med. 2015. PMID: 25799203 Free PMC article. No abstract available.
-
Terminally ill patients could benefit from stopping statins, study says.BMJ. 2015 Mar 23;350:h1620. doi: 10.1136/bmj.h1620. BMJ. 2015. PMID: 25801089 No abstract available.
-
Palliative care: Discontinuation of statins assessed.Nat Rev Cardiol. 2015 Jun;12(6):319. doi: 10.1038/nrcardio.2015.59. Epub 2015 Apr 14. Nat Rev Cardiol. 2015. PMID: 25869334 No abstract available.
-
ACP Journal Club: in palliative care, discontinuation of statins did not differ from continuation for mortality.Ann Intern Med. 2015 Aug 18;163(4):JC7. doi: 10.7326/ACPJC-2015-163-4-007. Ann Intern Med. 2015. PMID: 26280442 No abstract available.
-
Selecting the Optimal Design for Drug Discontinuation Trials in a Setting of Advanced, Life-Limiting Illness.JAMA Intern Med. 2015 Oct;175(10):1724-5. doi: 10.1001/jamainternmed.2015.3997. JAMA Intern Med. 2015. PMID: 26436748 No abstract available.
-
Selecting the Optimal Design for Drug Discontinuation Trials in a Setting of Advanced, Life-Limiting Illness.JAMA Intern Med. 2015 Oct;175(10):1725. doi: 10.1001/jamainternmed.2015.4000. JAMA Intern Med. 2015. PMID: 26436750 Free PMC article. No abstract available.
-
Selecting the Optimal Design for Drug Discontinuation Trials in a Setting of Advanced, Life-Limiting Illness-Reply.JAMA Intern Med. 2015 Oct;175(10):1725-6. doi: 10.1001/jamainternmed.2015.4003. JAMA Intern Med. 2015. PMID: 26436751 No abstract available.
-
Coding Error Resulting in Change in Secondary Outcome Scores in Trial of Safety and Benefit of Discontinuing Statin Therapy Among Terminally Ill Patients.JAMA Intern Med. 2019 Jan 1;179(1):126. doi: 10.1001/jamainternmed.2018.7162. JAMA Intern Med. 2019. PMID: 30508023 No abstract available.
References
-
- Currow DC, Stevenson JP, Abernethy AP, Plummer J, Shelby-James TM. Prescribing in palliative care as death approaches. J Am Geriatr Soc. 2007;55(4):590–595. - PubMed
-
- Holmes HM, Hayley DC, Alexander GC, Sachs GA. Reconsidering medication appropriateness for patients late in life. Arch Intern Med. 2006;166(6):605–609. - PubMed
-
- Vollrath AM, Sinclair C, Hallenbeck J. Discontinuing cardiovascular medications at the end of life: lipid-lowering agents. J Palliat Med. 2005;8(4):876–881. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
