

Evaluation of clinical risk factors to predict high on-treatment platelet reactivity and outcome in patients with stable coronary artery disease (PREDICT-STABLE)
- PMID: 25799149
- PMCID: PMC4370634
- DOI: 10.1371/journal.pone.0121620
Evaluation of clinical risk factors to predict high on-treatment platelet reactivity and outcome in patients with stable coronary artery disease (PREDICT-STABLE)
Abstract
Objectives: This study was designed to identify the multivariate effect of clinical risk factors on high on-treatment platelet reactivity (HPR) and 12 months major adverse events (MACE) under treatment with aspirin and clopidogrel in patients undergoing non-urgent percutaneous coronary intervention (PCI).
Methods: 739 consecutive patients with stable coronary artery disease (CAD) undergoing PCI were recruited. On-treatment platelet aggregation was tested by light transmittance aggregometry. Clinical risk factors and MACE during one-year follow-up were recorded. An independent population of 591 patients served as validation cohort.
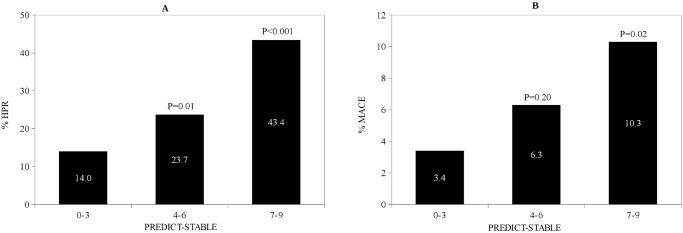
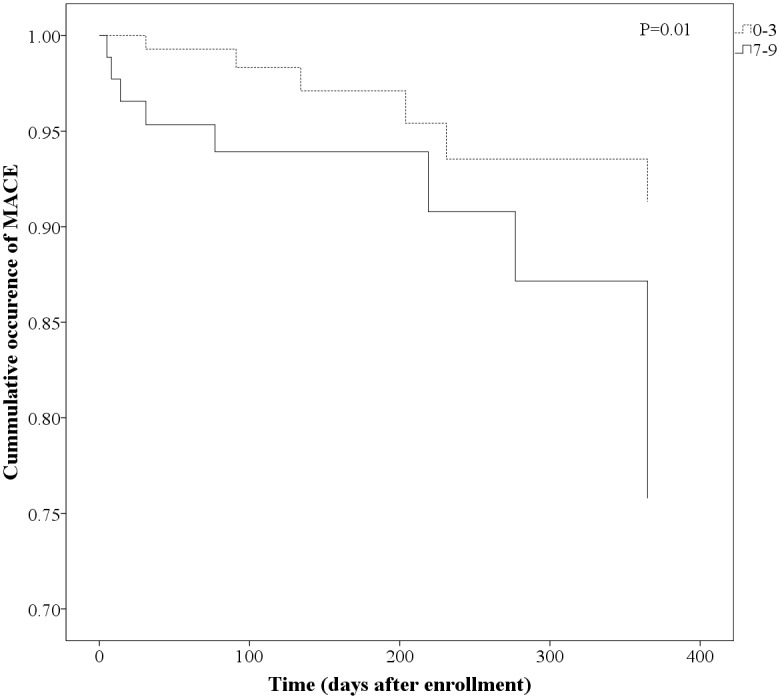
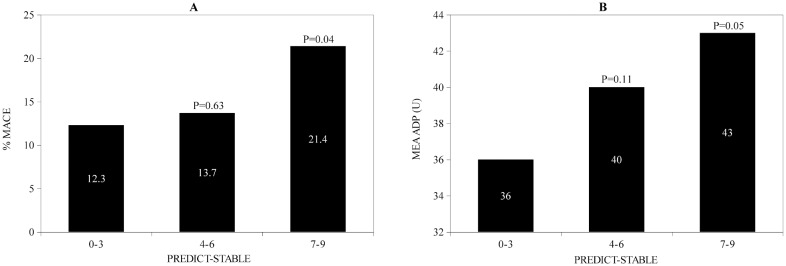
Results: Degree of on-treatment platelet aggregation was influenced by different clinical risk factors. In multivariate regression analysis older age, diabetes mellitus, elevated BMI, renal function and left ventricular ejection fraction were independent predictors of HPR. After weighing these variables according to their estimates in multivariate regression model, we developed a score to predict HPR in stable CAD patients undergoing elective PCI (PREDICT-STABLE Score, ranging 0-9). Patients with a high score were significantly more likely to develop MACE within one year of follow-up, 3.4% (score 0-3), 6.3% (score 4-6) and 10.3% (score 7-9); odds ratio 3.23, P=0.02 for score 7-9 vs. 0-3. This association was confirmed in the validation cohort.
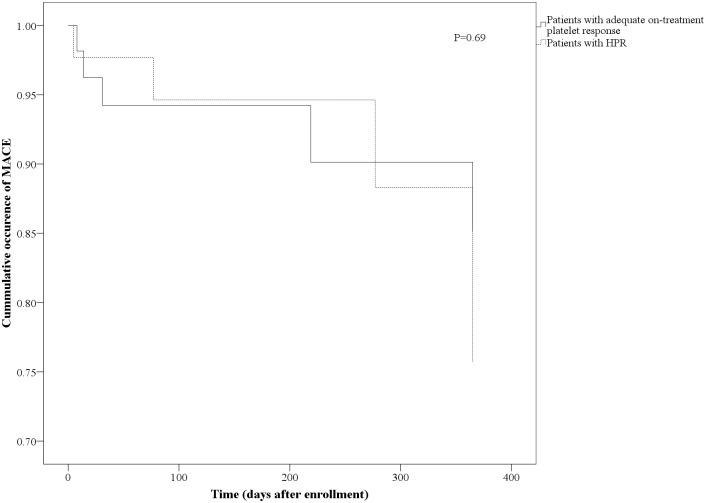
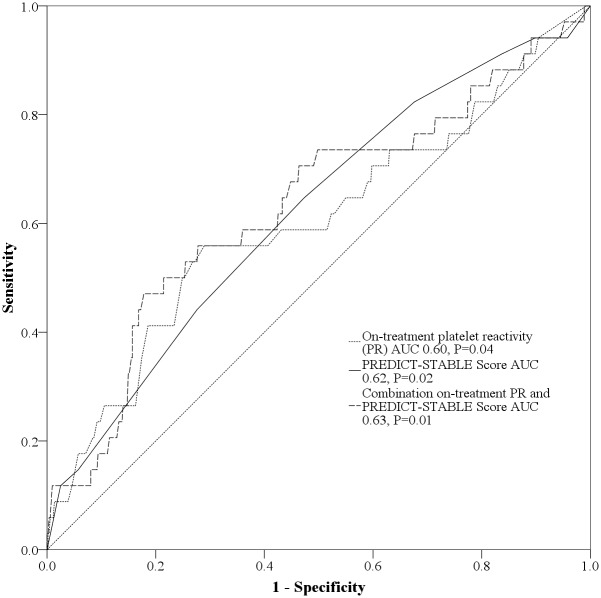
Conclusions: Variability of on-treatment platelet function and associated outcome is mainly influenced by clinical risk variables. Identification of high risk patients (e.g. with high PREDICT-STABLE score) might help to identify risk groups that benefit from more intensified antiplatelet regimen. Additional clinical risk factor assessment rather than isolated platelet function-guided approaches should be investigated in future to evaluate personalized antiplatelet therapy in stable CAD-patients.
Conflict of interest statement
Figures
References
-
- Gurbel PA, Bliden KP, Hiatt BL, O’Connor CM. Clopidogrel for coronary stenting: response variability, drug resistance, and the effect of pretreatment platelet reactivity. Circulation. 2003;107: 2908–2913. - PubMed
-
- Müller I, Besta F, Schulz C, Massberg S, Schönig A, Gawaz M. Prevalence of clopidogrel non-responders among patients with stable angina pectoris scheduled for elective coronary stent placement. Thromb Haemost. 2003;89: 783–787. - PubMed
-
- Serebruany VL, Steinhubl SR, Berger PB, Malinin AI, Bhatt DL, Topol EJ. Variability in platelet responsiveness to clopidogrel among 544 individuals. J Am Coll Cardiol. 2005;45: 246–251. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
