

Emergence of clonal hematopoiesis in the majority of patients with acquired aplastic anemia
- PMID: 25800665
- PMCID: PMC4433860
- DOI: 10.1016/j.cancergen.2015.01.007
Emergence of clonal hematopoiesis in the majority of patients with acquired aplastic anemia
Abstract
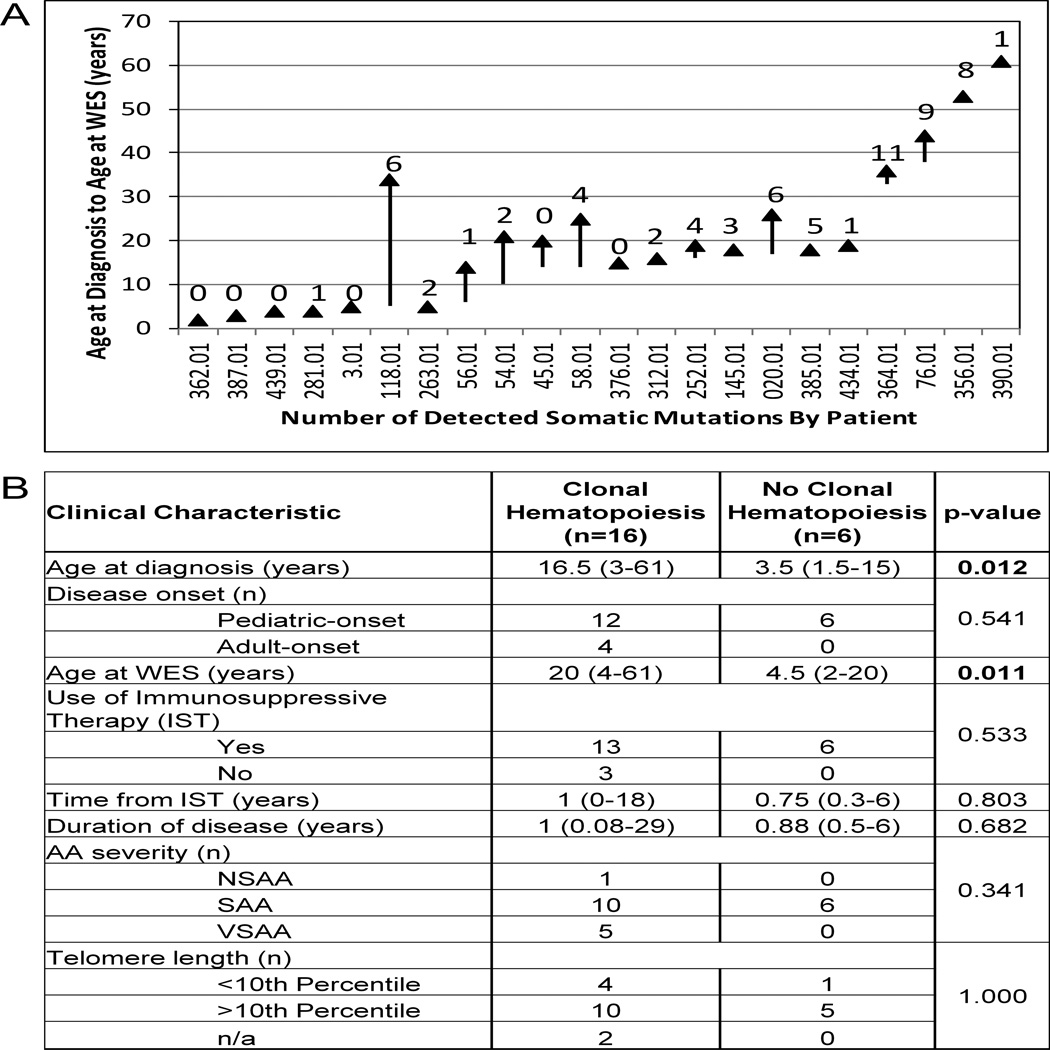
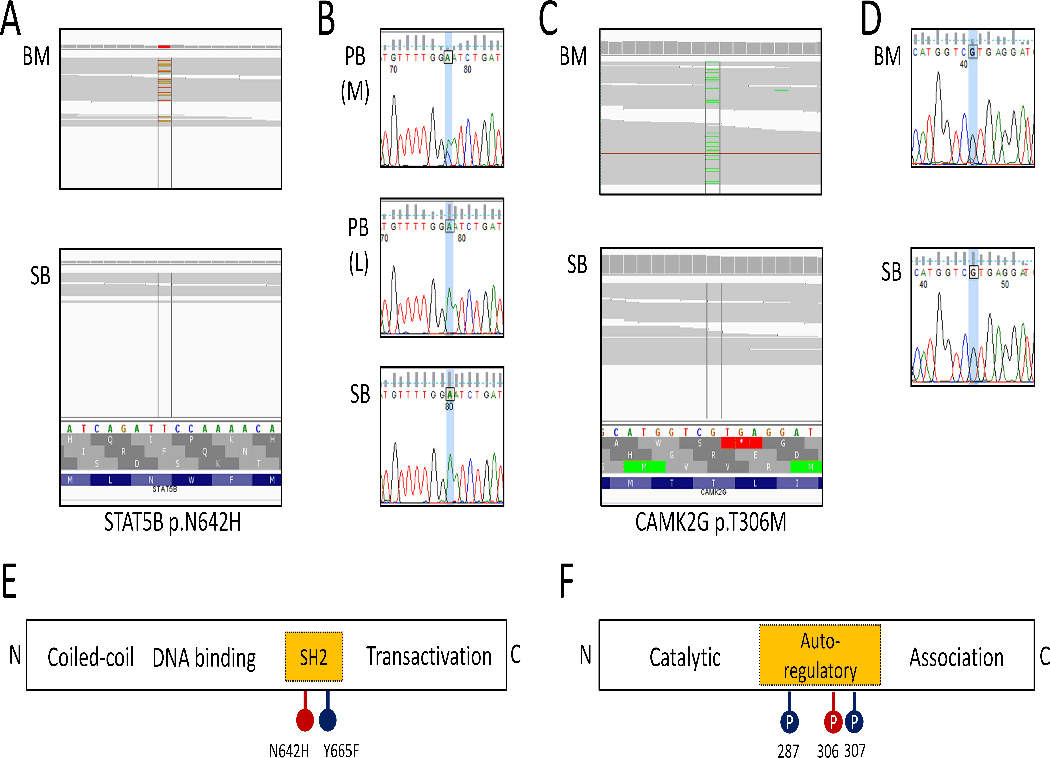
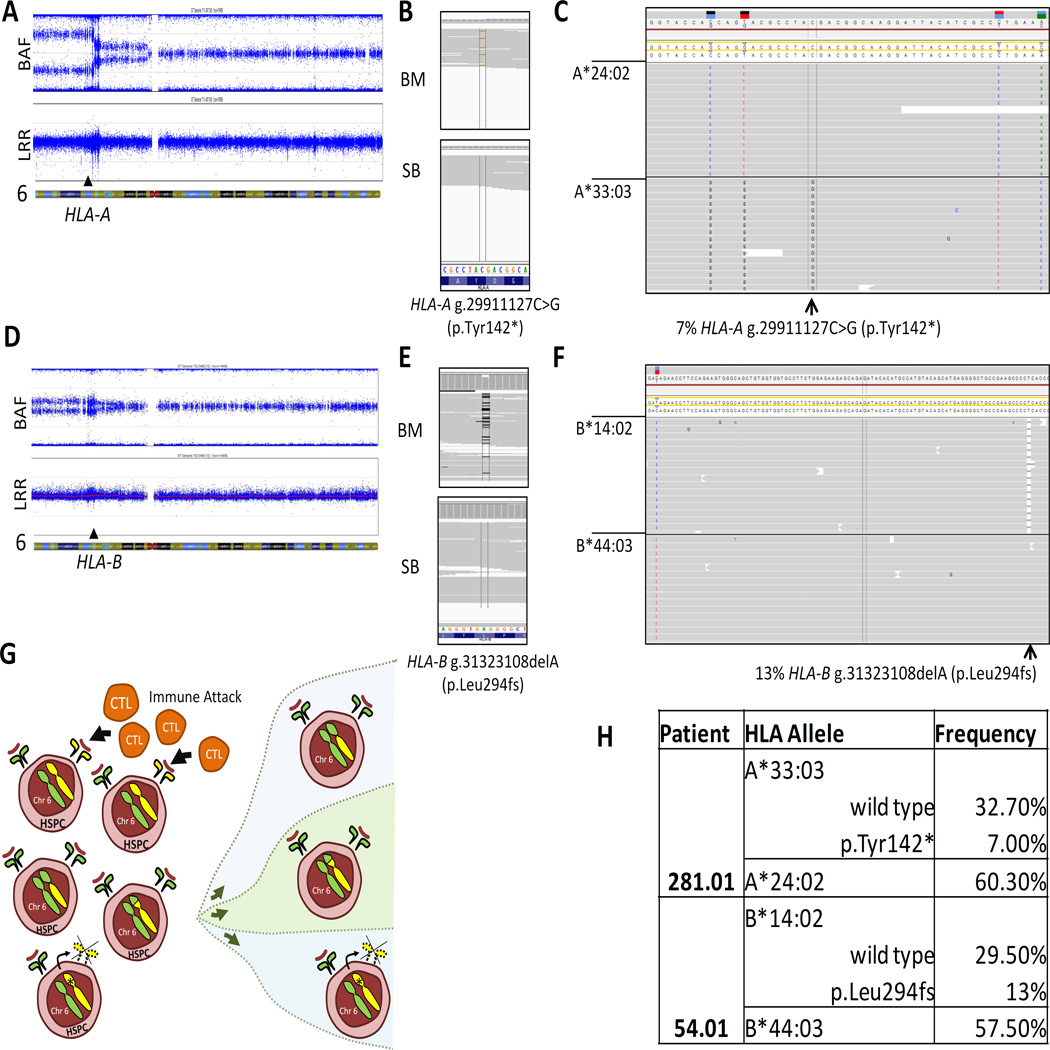
Acquired aplastic anemia (aAA) is a nonmalignant disease caused by autoimmune destruction of early hematopoietic cells. Clonal hematopoiesis is a late complication, seen in 20-25% of older patients. We hypothesized that clonal hematopoiesis in aAA is a more general phenomenon, which can arise early in disease, even in younger patients. To evaluate clonal hematopoiesis in aAA, we used comparative whole exome sequencing of paired bone marrow and skin samples in 22 patients. We found somatic mutations in 16 patients (72.7%) with a median disease duration of 1 year; of these, 12 (66.7%) were patients with pediatric-onset aAA. Fifty-eight mutations in 51 unique genes were found primarily in pathways of immunity and transcriptional regulation. Most frequently mutated was PIGA, with seven mutations. Only two mutations were in genes recurrently mutated in myelodysplastic syndrome. Two patients had oligoclonal loss of the HLA alleles, linking immune escape to clone emergence. Two patients had activating mutations in key signaling pathways (STAT5B (p.N642H) and CAMK2G (p.T306M)). Our results suggest that clonal hematopoiesis in aAA is common, with two mechanisms emerging-immune escape and increased proliferation. Our findings expand conceptual understanding of this nonneoplastic blood disorder. Future prospective studies of clonal hematopoiesis in aAA will be critical for understanding outcomes and for designing personalized treatment strategies.
Keywords: Clonal hematopoiesis; MDS; aplastic anemia; bone marrow failure; myelodysplastic syndrome.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- Young NS, Maciejewski J. The pathophysiology of acquired aplastic anemia. N Engl J Med. 1997;336:1365–1372. - PubMed
-
- Socie G, Henry-Amar M, Bacigalupo A, Hows J, Tichelli A, Ljungman P, McCann SR, Frickhofen N, Van't Veer-Korthof E, Gluckman E. Malignant tumors occurring after treatment of aplastic anemia. European Bone Marrow Transplantation-Severe Aplastic Anaemia Working Party. N Engl J Med. 1993;329:1152–1157. - PubMed
-
- Young NS, Maciejewski JP, Sloand E, Chen G, Zeng W, Risitano A, Miyazato A. The relationship of aplastic anemia and PNH. Int J Hematol. 2002;76(Suppl 2):168–172. - PubMed
-
- Dunn DE, Tanawattanacharoen P, Boccuni P, Nagakura S, Green SW, Kirby MR, Kumar MS, Rosenfeld S, Young NS. Paroxysmal nocturnal hemoglobinuria cells in patients with bone marrow failure syndromes. Ann Intern Med. 1999;131:401–408. - PubMed
-
- Katagiri T, Sato-Otsubo A, Kashiwase K, Morishima S, Sato Y, Mori Y, Kato M, Sanada M, Morishima Y, Hosokawa K, Sasaki Y, Ohtake S, Ogawa S, Nakao S. Frequent loss of HLA alleles associated with copy number-neutral 6pLOH in acquired aplastic anemia. Blood. 2011;118:6601–6609. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
Grants and funding
- T32 GM008638/GM/NIGMS NIH HHS/United States
- T32 HL007439/HL/NHLBI NIH HHS/United States
- R01 HL097064/HL/NHLBI NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1TR000003/TR/NCATS NIH HHS/United States
- K08 HL122306/HL/NHLBI NIH HHS/United States
- 5-T32-HL-07439-34/HL/NHLBI NIH HHS/United States
- R01 CA105312/CA/NCI NIH HHS/United States
- R24DK103001/DK/NIDDK NIH HHS/United States
- T32-GM008638/GM/NIGMS NIH HHS/United States
- P30 CA016520/CA/NCI NIH HHS/United States
- K12 HL087064/HL/NHLBI NIH HHS/United States
- K12 HL097064/HL/NHLBI NIH HHS/United States
- R24 DK103001/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
