

Survival, Durable Response, and Long-Term Safety in Patients With Previously Treated Advanced Renal Cell Carcinoma Receiving Nivolumab
- PMID: 25800770
- PMCID: PMC4517051
- DOI: 10.1200/JCO.2014.58.1041
Survival, Durable Response, and Long-Term Safety in Patients With Previously Treated Advanced Renal Cell Carcinoma Receiving Nivolumab
Abstract
Purpose: Blockade of the programmed death-1 inhibitory cell-surface molecule on immune cells using the fully human immunoglobulin G4 antibody nivolumab mediates tumor regression in a portion of patients with advanced treatment-refractory solid tumors. We report clinical activity, survival, and long-term safety in patients with advanced renal cell carcinoma (RCC) treated with nivolumab in a phase I study with expansion cohorts.
Patients and methods: A total of 34 patients with previously treated advanced RCC, enrolled between 2008 and 2012, received intravenous nivolumab (1 or 10 mg/kg) in an outpatient setting once every two weeks for up to 96 weeks and were observed for survival and duration of response after treatment discontinuation.
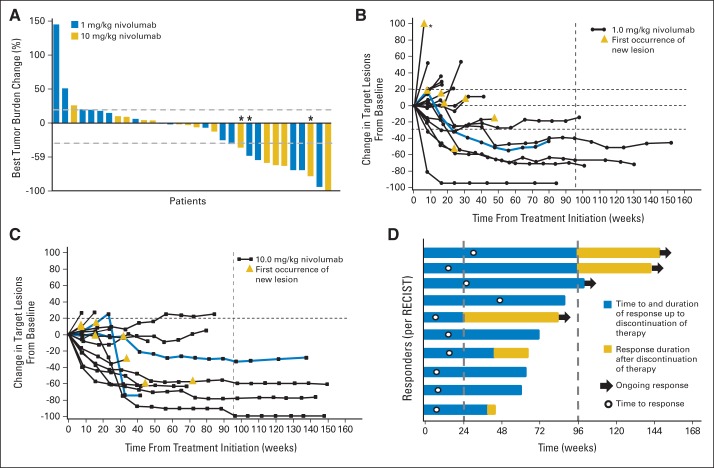
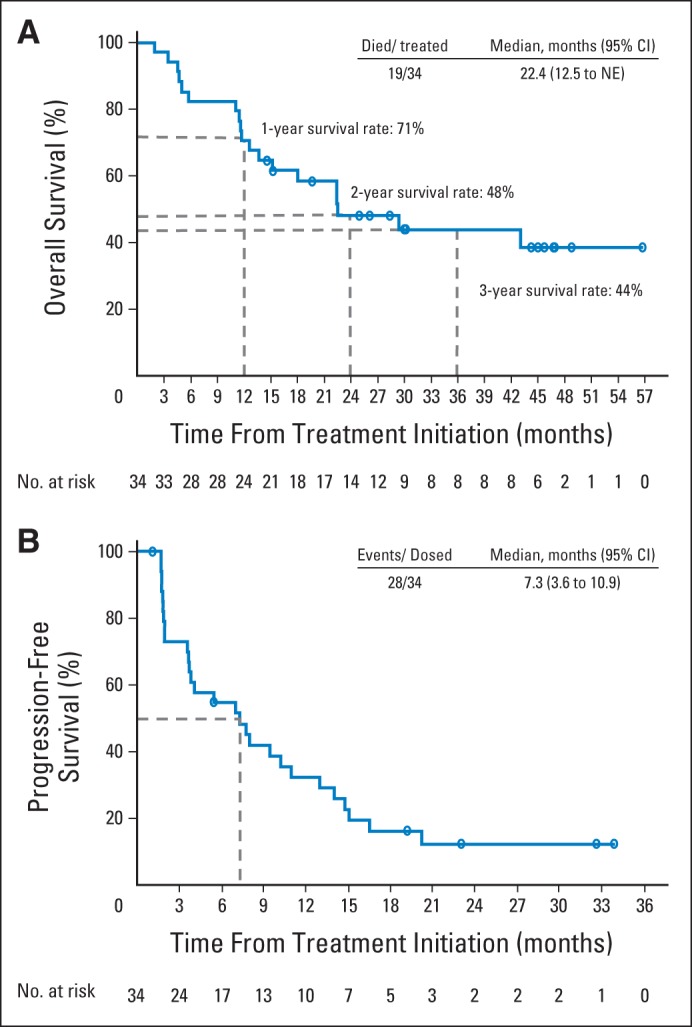
Results: Ten patients (29%) achieved objective responses (according to RECIST [version 1.0]), with median response duration of 12.9 months; nine additional patients (27%) demonstrated stable disease lasting > 24 weeks. Three of five patients who stopped treatment while in response continued to respond for ≥ 45 weeks. Median overall survival in all patients (71% with two to five prior systemic therapies) was 22.4 months; 1-, 2-, and 3-year survival rates were 71%, 48%, and 44%, respectively. Grade 3 to 4 treatment-related adverse events occurred in 18% of patients; all were reversible.
Conclusion: Patients with advanced treatment-refractory RCC treated with nivolumab demonstrated durable responses that in some responders persisted after drug discontinuation. Overall survival is encouraging, and toxicities were generally manageable. Ongoing randomized clinical trials will further assess the impact of nivolumab on overall survival in patients with advanced RCC.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
Durable Responses With PD-1 Inhibition in Lung and Kidney Cancer and the Ongoing Search for Predictive Biomarkers.J Clin Oncol. 2015 Jun 20;33(18):1993-4. doi: 10.1200/JCO.2015.61.4172. Epub 2015 Apr 27. J Clin Oncol. 2015. PMID: 25918290 No abstract available.
References
-
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115–124. - PubMed
-
- Escudier B, Pluzanska A, Koralewski P, et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: A randomised, double-blind phase III trial. Lancet. 2007;370:210–2111. - PubMed
-
- Escudier B, Eisen T, Stadler WM, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007;356:125–134. - PubMed
-
- Hudes G, Carducci M, Tomczak P, et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med. 2007;356:2271–2281. - PubMed
-
- McDermott DF, Regan MM, Clark JI, et al. Randomized phase III trial of high-dose interleukin-2 versus subcutaneous interleukin-2 and interferon in patients with metastatic renal cell carcinoma. J Clin Oncol. 2005;23:133–141. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
