

What does delirium cost? An economic evaluation of hyperactive delirium
- PMID: 25801513
- PMCID: PMC4715123
- DOI: 10.1007/s00391-015-0871-6
What does delirium cost? An economic evaluation of hyperactive delirium
Abstract
Background: Demographic changes have resulted in an increase in the number of older (> 75 years) multimorbid patients in clinics. In addition to the primary acute diagnoses that lead to hospitalization, this group of patients often has cognitive dysfunctions, such as delirium. According to clinical experience, delirium patients are more time-consuming for clinicians and their function is often poor. The costs caused by delirium patients are currently unknown. In the present study, a retrospective examination of a database was carried out to calculate the costs that arise during the clinical treatment of documented delirium patients.
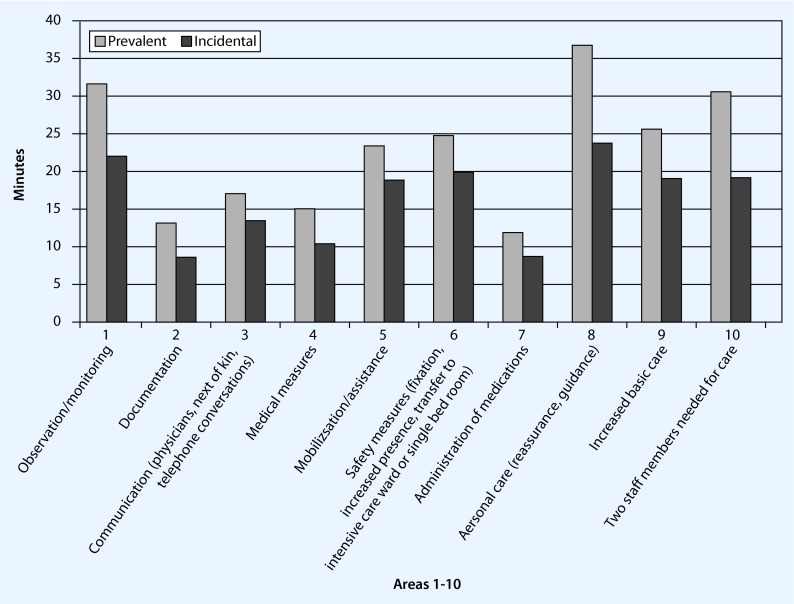
Setting and methods: The purpose of this retrospective analysis was to collect information recorded by nursing personnel trained in the treatment of delirium and information from a manual documentation matrix for additional time expenditure. In the database analysis anonymous data of previously discharged patients for a time window of 3 months were analyzed. Documented additional expenditure for patients with hyperactive delirium at hospitalization were analyzed by personnel. Material costs, the duration of hospitalization by main diagnosis and age clusters during hospitalization until discharge were also examined. The analysis was performed in a hospital with internal wards.
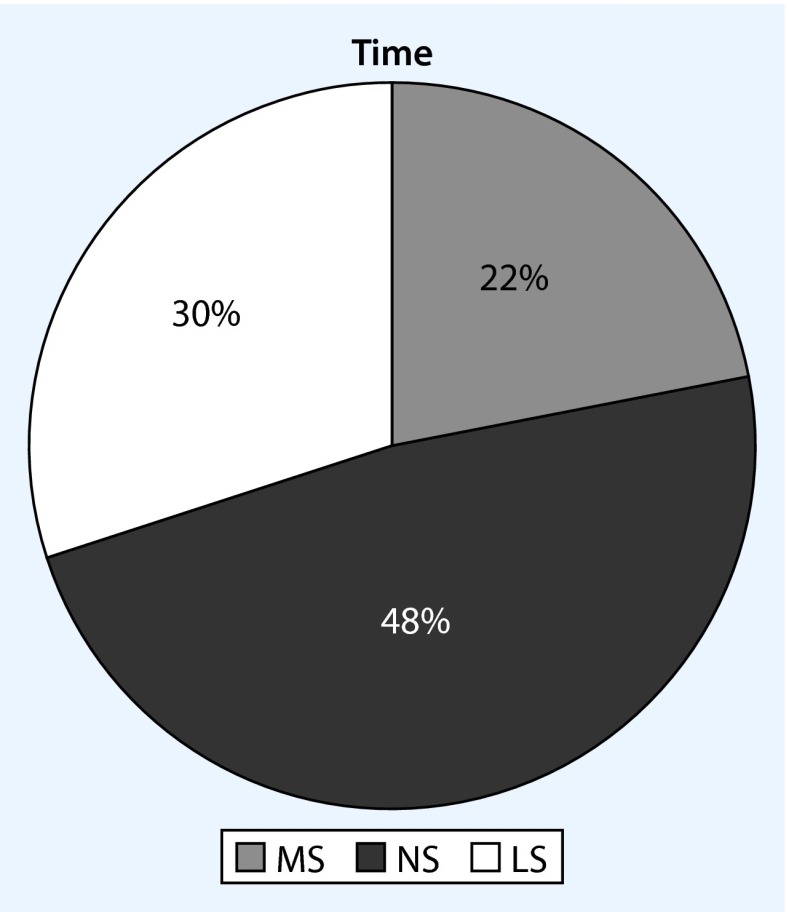
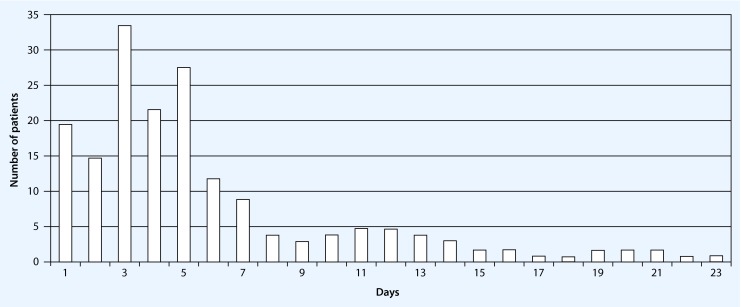
Results: Data for 82 hyperactive delirium patients were examined and an average of approximately 240 min of additional personnel expenditure for these patients was found. These patients were approximately 10 years older (p < 0.01) and were hospitalized for an average of 4.2 days longer (p < 0.01) than non-delirium patients. Hyperactive delirium usually developed within the first 5 days of hospitalization and lasted 1.6 days on average. Patients for whom hyperactive delirium was detected early were hospitalized for significantly less time than those for whom it was detected late (6.85 versus 13.61 days, p = 0.002). Additionally, calculated personnel and material costs, including costs affecting the hospitalization period, amounted to approximately 1200 € per hyperactive delirium patient. This corresponds to approximately 0.3 CMP (casemix points) per patient.
Conclusion: The calculations of personnel and material costs and duration of hospitalization in patients with hyperactive delirium demonstrated significant additional costs. Early routine detection of delirium can be achieved through training and this approach leads to a shortening of the hospitalization period and lower costs.
Hintergrund: Die demografischen Veränderungen führen zu mehr hochbetagten (> 75 Jahre), multimorbiden Patienten in der Klinik. Diese Patientengruppe zeigt neben den akuten Einweisungshauptdiagnosen (HD) häufig kognitive Funktionsstörungen, z. B. ein Delir. Klinischer Erfahrung zufolge sind Delirpatienten aufwendiger, oft sind sie funktionell stark beeinträchtigt. Wie viel Delirpatienten an Kosten verursachen, ist bisher nicht bekannt. In der vorliegenden Arbeit wurde retrospektiv berechnet, welche Kosten bei der klinischen Versorgung dokumentierter Delirpatienten anfielen.
Setting und Methoden: Grundlage für diese retrospektive Auswertung war speziell auf die Erfassung von Delirien geschultes Pflegepersonal und eine händische Dokumentationsmatrix für zusätzlichen Zeitaufwand. In der Datenbankanalyse wurden die anonymisierten Daten von bereits entlassenen Patienten einer allgemeinen Innere Abteilung in einem Krankenhaus der Grund- und Regelversorgung aus einem Zeitfenster von 3 Monaten ausgewertet. Bei Vorliegen von hypermotorischen Delirien in der Aufnahmesituation bzw. im klinischen Verlauf bis zur Entlassung wurden die dokumentierten Zusatzaufwände hinsichtlich Personal, Material und Verweildauer nach HD und Altersclustern ausgewertet.
Ergebnisse: Untersucht wurden Daten von 82 hypermotorischen Delirpatienten, die durchschnittlich etwa 240 Minuten an zusätzlichem Personalaufwand benötigten. Diese Patienten waren gegenüber Nicht-Delirpatienten etwa 10 Jahre älter (p < 0,01) und lagen im Durchschnitt 4,2 Tage länger (p < 0,01) im Krankenhaus. Hypermotorische Delirien traten meist innerhalb der ersten 5 Tage auf und dauerten durchschnittlich 1,6 Tage; bei früh diagnostiziertem Delir signifikant kürzer als bei spät erkanntem (6,85 vs. 13,61 Tage; p = 0,002). Zusätzlich errechnete Personal- und Sachkosten beliefen sich einschließlich der Verweildauerbeeinflussung auf etwa EUR 1200,00 pro hypermotorischem Delirpatienten, entsprechend etwa 0,3 CMP pro Patient.
Schlussfolgerung: Die Kalkulation der Bereiche Personal, Sachkosten und Verweildauer bei Patienten mit hypermotorischen Delirien zeigt die erheblichen Zusatzkosten bei Delirpatienten auf. Eine frühe, routinemäßige Erfassung von Delirien kann durch eine Schulung erfolgreich gelingen, führt zu spezifischen Prozessen, verkürzt die Verweildauer und senkt die Kosten.
Keywords: Costs; Delirium; Hospitalization period; Personnel expenses.
Conflict of interest statement
W. Weinrebe, E. Johannsdottir, M. Karaman and I. Füsgen state that there are no conflicts of interest.
Figures
References
-
- Han JH, Wilson A, Vasilevskis EE, Shintani A, Schnelle JF, Dittus RS, Graves AJ, Storrow AB, Shuster J, Ely EW. Diagnosing delirium in older emergency department patients: validity and reliability of the delirium triage screen and the brief confusion assessment method. Ann Emerg Med. 2013;62(5):457–465. doi: 10.1016/j.annemergmed.2013.05.003. - DOI - PMC - PubMed
-
- http://www.bpb.de/wissen/VCKSHL,0,Ausgaben%20der_Krankenhäuser, www.gbe-bund.de; Statistisches Bundesamt: Gesundheitsausgaben 2013
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
