

Trends in susceptibility of Escherichia coli from intra-abdominal infections to ertapenem and comparators in the United States according to data from the SMART program, 2009 to 2013
- PMID: 25801558
- PMCID: PMC4432174
- DOI: 10.1128/AAC.05186-14
Trends in susceptibility of Escherichia coli from intra-abdominal infections to ertapenem and comparators in the United States according to data from the SMART program, 2009 to 2013
Abstract
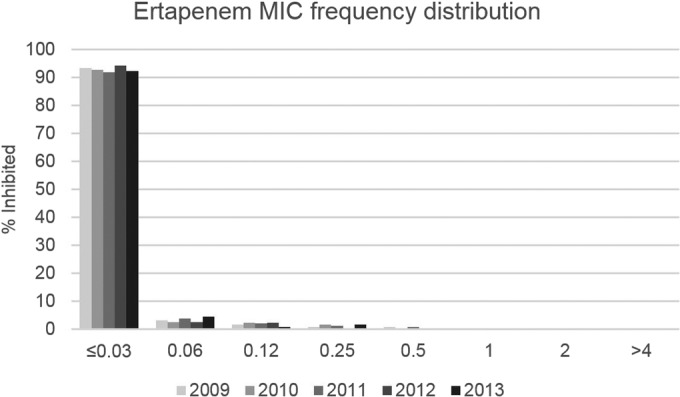
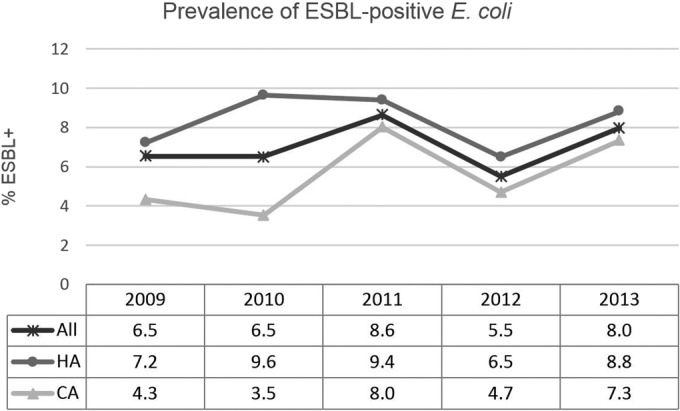
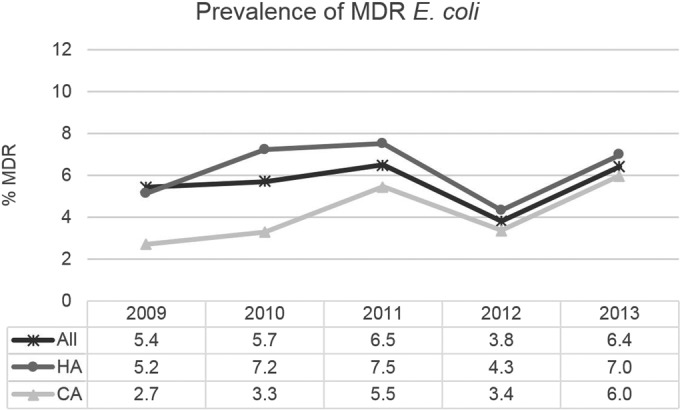
Antimicrobial resistance in Enterobacteriaceae, including resistance to carbapenems, is increasing worldwide. However, using U.S. Study for Monitoring Antimicrobial Resistance Trends (SMART) data for 2009 to 2013, no statistically significant decreasing susceptibility trends were found overall for Escherichia coli isolates from patients with intra-abdominal infections. In the subset of isolates from community-associated infections, susceptibility to levofloxacin decreased significantly and the increasing rate of multidrug-resistant E. coli approached statistical significance. In 2013, ertapenem, imipenem, and amikacin showed the highest susceptibility rates (≥99%) and fluoroquinolones the lowest (<70%). The 10 non-ertapenem-susceptible isolates (0.3% of all E. coli isolates) encoded one or more carbapenemases, extended-spectrum β-lactamases (ESBLs), AmpC β-lactamases, or non-ESBL β-lactamases.
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Vardakas KZ, Tansarli GS, Petros I, Rafailidis PI, Falagas ME. 2012. Carbapenems versus alternative antibiotics for the treatment of bacteraemia due to Enterobacteriaceae producing extended-spectrum β-lactamases: a systematic review and meta-analysis. J Antimicrob Chemother 67:2793–2803. doi:10.1093/jac/dks301. - DOI - PubMed
-
- Solomkin JS, Mazuski JE, Bradley JS, Rodvold KA, Goldstein EJC, Baron EJ, O'Neill PJ, Chow AW, Patchen Dellinger E, Eachempai SR, Gorbach S, Hilfiker M, May AK, Nathens AB, Sawyer RG, Bartlett JG. 2010. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Surg Infect 11:79–109. doi:10.1089/sur.2009.9930. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
