

The complement system and adverse pregnancy outcomes
- PMID: 25802092
- PMCID: PMC4447554
- DOI: 10.1016/j.molimm.2015.02.030
The complement system and adverse pregnancy outcomes
Abstract
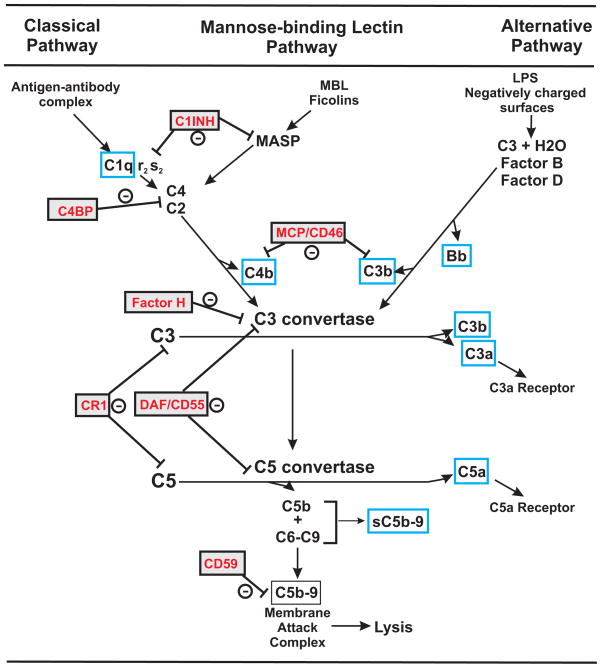
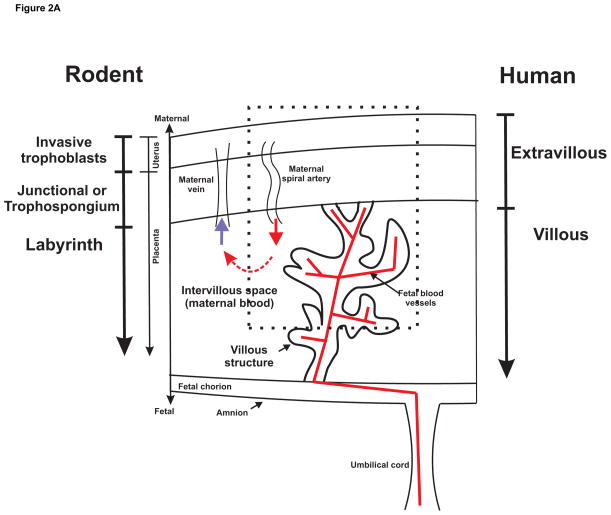
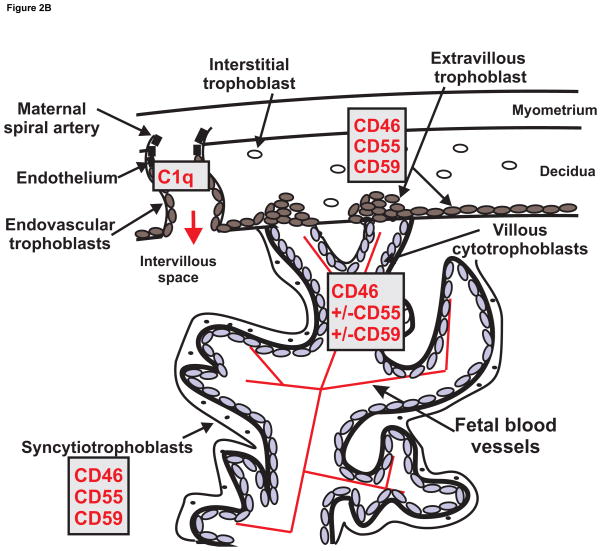
Adverse pregnancy outcomes significantly contribute to morbidity and mortality for mother and child, with lifelong health consequences for both. The innate and adaptive immune system must be regulated to insure survival of the fetal allograft, and the complement system is no exception. An intact complement system optimizes placental development and function and is essential to maintain host defense and fetal survival. Complement regulation is apparent at the placental interface from early pregnancy with some degree of complement activation occurring normally throughout gestation. However, a number of pregnancy complications including early pregnancy loss, fetal growth restriction, hypertensive disorders of pregnancy and preterm birth are associated with excessive or misdirected complement activation, and are more frequent in women with inherited or acquired complement system disorders or complement gene mutations. Clinical studies employing complement biomarkers in plasma and urine implicate dysregulated complement activation in components of each of the adverse pregnancy outcomes. In addition, mechanistic studies in rat and mouse models of adverse pregnancy outcomes address the complement pathways or activation products of importance and allow critical analysis of the pathophysiology. Targeted complement therapeutics are already in use to control adverse pregnancy outcomes in select situations. A clearer understanding of the role of the complement system in both normal pregnancy and complicated or failed pregnancy will allow a rational approach to future therapeutic strategies for manipulating complement with the goal of mitigating adverse pregnancy outcomes, preserving host defense, and improving long term outcomes for both mother and child.
Keywords: Complement system; Fetal growth restriction; Miscarriage; Placenta; Preeclampsia; Pregnancy; Preterm birth.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors have no conflicts to report.
Figures
References
-
- ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33. Obstet Gynecol. 2002 Jan;99:159–67. - PubMed
-
- ACOG. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122:1122–31. - PubMed
-
- Agostinis C, Bulla R, Tripodo C, Gismondi A, Stabile H, Bossi F, Guarnotta C, Garlanda C, De Seta F, Spessotto P, Santoni A, Ghebrehiwet B, Girardi G, Tedesco F. An alternative role of C1q in cell migration and tissue remodeling: contribution to trophoblast invasion and placental development. J Immunol. 2010;185:4420–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
