

Effect of low-dose glucocorticoid on corticosteroid insufficient patients with acute exacerbation of chronic obstructive pulmonary disease
- PMID: 25802564
- PMCID: PMC4369528
- DOI: 10.5847/wjem.j.1920-8642.2015.01.006
Effect of low-dose glucocorticoid on corticosteroid insufficient patients with acute exacerbation of chronic obstructive pulmonary disease
Abstract
Background: This study aimed to investigate the prevalence rate of critical illness-related corticosteroid insufficiency (CIRCI) and the effect of low-dose glucocorticoid on prognosis of CIRCI in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD).
Methods: Since January 2010 to December 2012, 385 patients, who met the criteria of AECOPD, were enrolled in the Intensive Care Unit (ICU) of the First People's Hospital and Municipal Central Hospital of Xiangtan City. The AECOPD patients complicated with CIRCI screened by an adrenalcorticotrophic hormone test within 12 hours after admission to ICU were divided into a treatment group (n=32) and a control group (n=31) for a prospective, randomized and controlled clinical trial. Hydrocortisone (150 mg/d) or normal saline was injected intravenously for 7 days. The patients were followed up for 28 days after injection. The endpoint included 28-day survival time, non-shock time, ICU stay and the period of non-mechanical ventilation. The markers of inflammation C-reactive protein, tumor necrosis factor-α, interleukin 6 and procalcitonin were measured at baseline and 7 days after treatment. The variables were analyzed by Student's t test, the non-parametric statistical test, the Chi-square test or the Kaplan-Meier method with SPSS18.0 statistic software. A P value <0.05 was considered statistically significant.
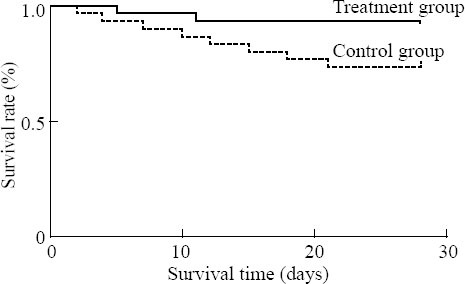
Results: Totally 63 patients were diagnosed with CIRCI by an adrenalcorticotrophic hormone test and the prevalence rate was 16.4%. The shock rate of the AECOPD patients complicated with CIRCI was higher than that of the AECOPD patients without CIRCI (23.8% vs. 8.7%, P<0.01). Kaplan-Meier analysis revealed that the 28-day survival time of the treatment group was obviously longer than that of the control group (P<0.05). Compared with the control group, shock-free days within 28 days was longer in the treatment group (18.2±9.5 vs. 25.8±4.1, P<0.05). Treatment with low-dose glucocorticoid obviously decreased the markers of infection and inflammation (P<0.01), such as C-reactive protein (13.2±5.5 mg/L vs. 8.3±3.1 mg/L for the control group; 13.5±5.9 mg/L vs. 5.1±2.3 mg/L for the treatment group), tumor necrosis factor-α (26.1±16.2 μg/L vs. 17.5±11.7 μg/L for the control group; 25.0±14.8 μg/L vs. 10.4±7.8 μg/L for the treatment group) and procalcitonin (3.88 μg/L vs. 2.03 μg/L for the control group; 3.77 μg/L vs. 1.26 μg/L for the treatment group). Furthermore, the markers in the treatment group decreased more obviously than those in the control group (P<0.01).
Conclusion: The prevalence rate of CIRCI was higher in the patients with AECOPD in the department of critical medicine, and low-dose glucocorticoid treatment for one week reduced the 28-day mortality, shock time and markers of infection and inflammation.
Keywords: Acute exacerbation; Chronic obstructive pulmonary disease; Corticosteroid insufficiency; Critical illness; Glucocorticoid; Inflammation; Prevalence rate; Prognosis.
Conflict of interest statement
Figures
References
-
- Marik PE, Pastores SM, Annane D, Meduri GU, Sprung CL, Arlt W, et al. Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: consensus statements from an international task force by the American College of Critical Care Medicine. Crit Care Med. 2008;36:1937–1949. - PubMed
-
- Annane D, Sébille V, Charpentier C, Bollaert PE, François B, Korach JM, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002;288:862–871. - PubMed
-
- Liu L, Li J, Huang YZ, Liu SQ, Yang CS, Guo FM, et al. The effect of stress dose glucocorticoid on patients with acute respiratory distress syndrome combined with critical illness-related corticosteroid insufficiency. Zhonghua Nei Ke Za Zhi. 2012;51:599–603. - PubMed
-
- Zhang YC, Zhang SJ, Teng GL, Tian GL, Xu L, Cao RF, et al. Adrenal insufficiency evaluation by using low-dose ACTH stimulation test in critical illness children. Zhonghua Er Ke Za Zhi. 2012;21:472–477.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous