

The Evolution and Advancement of Endoscopic Foraminal Surgery: One Surgeon's Experience Incorporating Adjunctive Techologies
- PMID: 25802587
- PMCID: PMC4365579
- DOI: 10.1016/SASJ-2006-0014-RR
The Evolution and Advancement of Endoscopic Foraminal Surgery: One Surgeon's Experience Incorporating Adjunctive Techologies
Abstract
Background: Endoscopic spine surgery has evolved gradually through improvements in endoscope design, instrumentation, and surgical techniques. The ability to visualize and treat painful pathology endoscopically through the foramen has opened the door for the diagnosis and treatment of degenerative conditions of the lumbar spine (from T10 to S1). Other endoscopic techniques for treating a painful disc have been focused on a posterior approach and has been compared with micro-lumbar discectomy. These procedures have not been more effective than open microdiscectomy but are less invasive, have less surgical morbidity, and allow for more rapid surgical recovery. Spinal decompression and fusion was the fallback procedure when nonsurgical treatment or discectomy failed to relieve sciatica and back pain. Foraminal endoscopic surgery, however, provides a truly minimally invasive alternative approach to the pathoanatomy of the lumbar spine because it preserves the multifidus muscle, maintains motion, and eliminates or, at worst, delays the need for fusion.
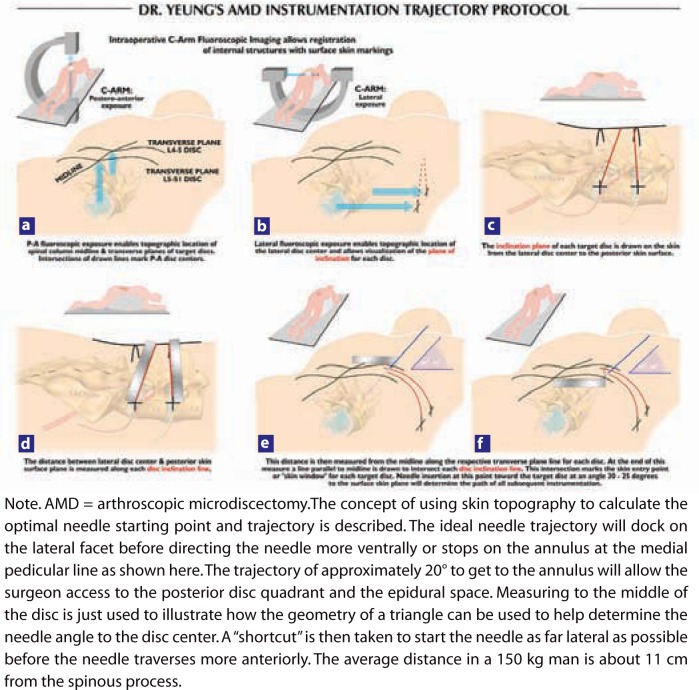
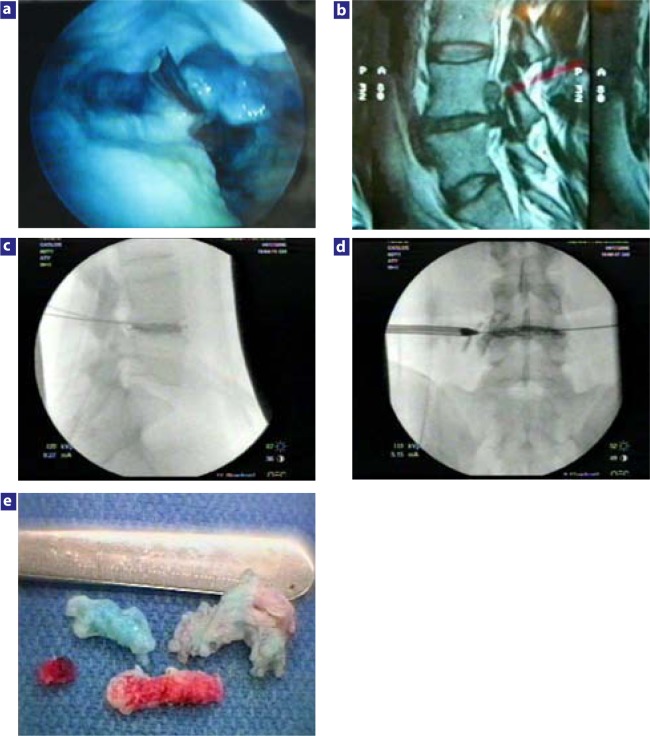
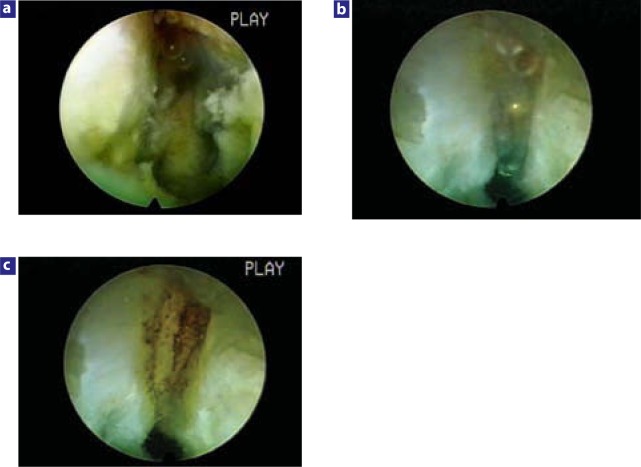
Methods: The following developments helped facilitate the evolution of a transforaminal endoscopic surgery procedure for disc herniations from a foraminal disc decompression, also known as percutaneous endoscopic lumbar discectomy, to a more complete foraminal surgical technique that can address spinal stenosis and spinal instability. This expanded capability gives foraminal endoscopic surgery distinct advantages and flexibility for certain painful degenerative conditions compared with open surgery. Advancement of the technique occurred when needle trajectory and placement was refined to better target each type of herniation with precise needle and cannula positioning directed at the herniation. New instrumentation and inclusion of a biportal technique also facilitated removal of extruded, migrated, and sequestered disc herniations. The further development of foraminoscopes with larger working channels and high speed burrs to remove bone more efficiently, along with recognition of foraminal pathoanatomy in the foramen, led to the identification and treatment of other painful degenerative conditions of the lumbar spine such as failed back surgery syndrome, recurrent disc herniations, lateral foraminal stenosis, degenerative spondylolisthesis, and isthmic spondylolisthesis. A summary of the endoscopic techniques currently used and trademarked by the author as the YESS technique include: (1) a published protocol for optimal needle and instrument placement calculated by lines drawn on the skin from the C-arm image; (2) evocative chromodiscography by the operating surgeon with nonionic radiologic contrast and indigo carmine dye to confirm concordant pain production and to stain tissue in contact with the injectate; (3) selective endoscopic discectomy, which targets the removal of loose degenerative nucleus stained differentially by indigo carmine dye; (4) thermal annuloplasty, a visualized radiofrequency thermal modulation of disc and annular defects guided by vital tissue staining; (5) endoscopic foraminoplasty, a decompression of the lateral and subarticular recess, including disc and foraminal degenerative and isthmic spondylolisthesis; (6) visually and radiologically guided exploration of the epidural space; (7) probing the hidden zone of MacNab for normal nerves (and branches of spinal nerves known as furcal nerves) versus anomalous autonomic nerves in the foramen; and (8) a uniportal and biportal technique for inside-out removal of extruded and sequestered nucleus pulposus.
Results: Endoscopic foraminal surgical procedures are not limited to disc decompression. The approaches and techniques allow access to the lumbar spine for treatment of conditions ranging from discogenic pain to failed back surgery syndrome (most commonly caused by residual or recurrent disc herniation and lateral recess stenosis). More than 3000 patients have undergone endoscopic posterolateral surgical exploration and decompression by the author since 1991. The first 80 patients reported formed the basis for expansion of techniques as new instruments and adjunctive therapy methods were added to selective endoscopic discectomy and thermal annuloplasty. New anatomic and pathoanatomic conditions were reported as they were encountered.
Conclusions: New skills will become desirable and necessary for the spine surgeon to keep up with endoscopic technology in spine care. The emphasis is on visualization of painful pathoanatomy and preservation of mobility. A new focus is on nucleus replacement, annular repair, annular reinforcement, biologics, and even transforaminal interbody fusion as the procedure of last resort. The transforaminal surgical approach to the lumbar spine can allow for minimally invasive access without negatively affecting and destabilizing the multifidus muscle.
Keywords: Chymopapain; arthroscopic microdiscectomy; endoscopic foraminoplasty; endoscopic thermal annuloplasty; evocative chromodiscography; laser disc decompression; selective endoscopic discectomy.
Figures

References
-
- Dabezies EJ, Langford K, Morris J, Shields CB, Wilkinson HA. Safety and efficacy of chymopapain (Discase) in the treatment of sciatica due to a herniated nucleus pulposus. Results of a randomized, double-blind study. Spine. 1988;13:561–565. - PubMed
-
- Javid MJ, Nordby EJ, Ford LT, et al. Safety and efficacy of chymopapain (Chymodiactin) in herniated nucleus pulposus with sciatica. Results of a randomized, double-blind study. JAMA. 1983;249:2489–2494. - PubMed
-
- Hermantin FU, Peters T, Quartararo L, Kambin P. A prospective, randomized study comparing the results of open discectomy with those of video-assisted arthroscopic microdiscectomy. J Bone Joint Surg Am. 1999;81:958–965. - PubMed
-
- Mayer HM, Brock M. Percutaneous endoscopic discectomy: surgical technique and preliminary results compared to microsurgical discectomy. J Neurosurg. 1993;78:216–225. - PubMed
-
- Yeung AT. Spine: State of the Art Reviews. Vol. 7. Spine: State of the Art Reviews; 1993. Considerations for use of the KTP laser for disc decompression and ablation; pp. 67–93.
LinkOut - more resources
Full Text Sources
Research Materials