

Initial clinical experience with a next-generation artificial disc for the treatment of symptomatic degenerative cervical radiculopathy
- PMID: 25802644
- PMCID: PMC4365607
- DOI: 10.1016/j.esas.2010.01.002
Initial clinical experience with a next-generation artificial disc for the treatment of symptomatic degenerative cervical radiculopathy
Abstract
Background: A feasibility trial was conducted to evaluate the initial safety and clinical use of a next-generation artificial cervical disc (M6-C artificial cervical disc; Spinal Kinetics, Sunnyvale, CA) for the treatment of patients with symptomatic degenerative cervical radiculopathy. A standardized battery of validated outcome measures was utilized to assess condition-specific functional impairment, pain severity, and quality of life.
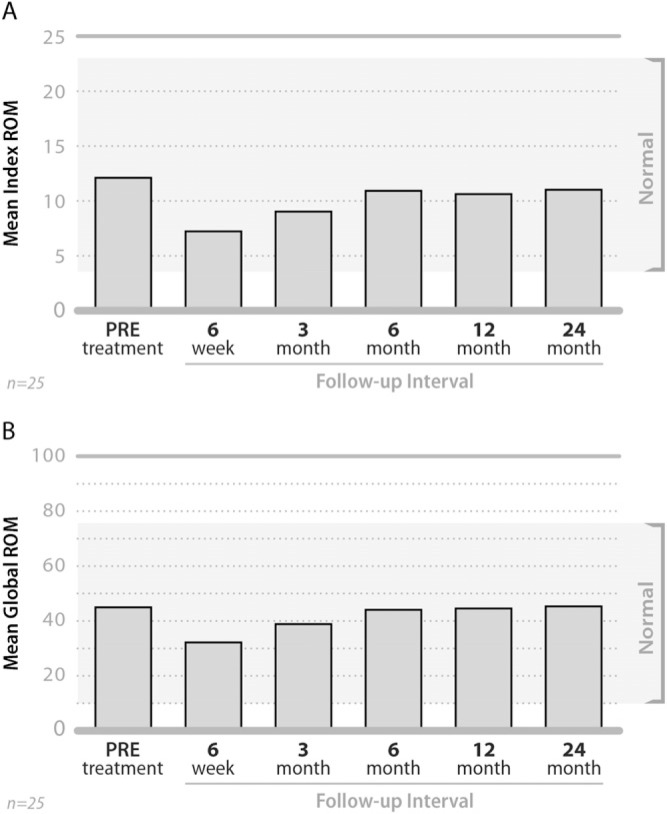
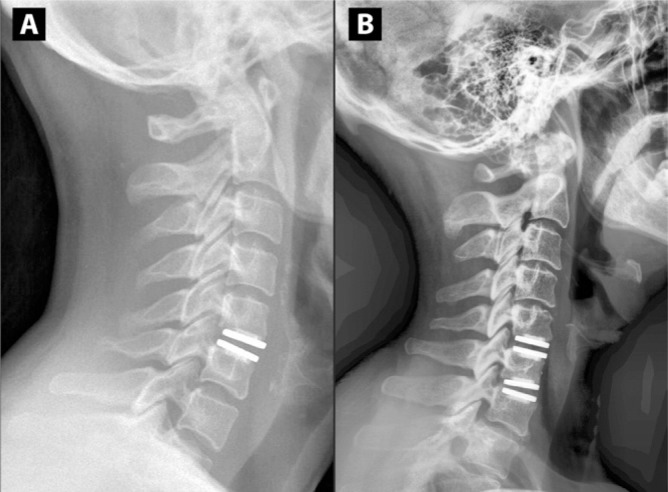
Methods: Thirty-six consecutive patients were implanted with the M6-C disc and complete clinical and radiographic outcomes for 25 patients (mean age, 44.5 ± 10.1 years) with radiographically-confirmed cervical disc disease and symptomatic radiculopathy unresponsive to conservative medical management are included in this report. All patients had disc-osteophyte complex causing neural compression and were treated with discectomy and artificial cervical disc replacement at either single level (n = 12) or 2-levels (n = 13). Functional impairment was evaluated using the Neck Disability Index (NDI). Evaluation of arm and neck pain severity utilized a standard 11-point numeric scale, and health-related quality of life was evaluated with the SF-36 Health Survey. Quantitative radiographic assessments of intervertebral motion were performed using specialized motion analysis software, QMA (Quantitative Motion Analysis; Medical Metrics, Houston, TX). All outcome measures were evaluated pre-treatment and at 6 weeks, 3, 6, 12, and 24 months.
Results: The mean NDI score improved from 51.6 ± 11.3% pre-treatment to 27.9 ± 16.9% at 24 months, representing an approximate 46% improvement (P <.0001). The mean arm pain score improved from 6.9 ± 2.5 pre-treatment to 3.9 ± 3.1 at 24 months (43%, P =.0006). The mean neck pain score improved from 7.8 ± 2.0 pre-treatment to 3.8 ± 3.0 at 24 months (51%, P <.0001). The mean PCS score of the SF-36 improved from 34.8 ± 7.8 pre-treatment to 43.8 ± 9.3 by 24 months (26%, P =.0006). Subgroup analyses found that patients treated at single level and those with a shorter duration of symptoms showed better functional results. By 24 months, the mean range of motion (ROM) value at the treated level had returned to approximately pretreatment levels (12.2° vs 11.1°). There were no serious device-related adverse events, surgical re-interventions or radiographic evidence of heterotopic ossification, device migration, or expulsion in this study group.
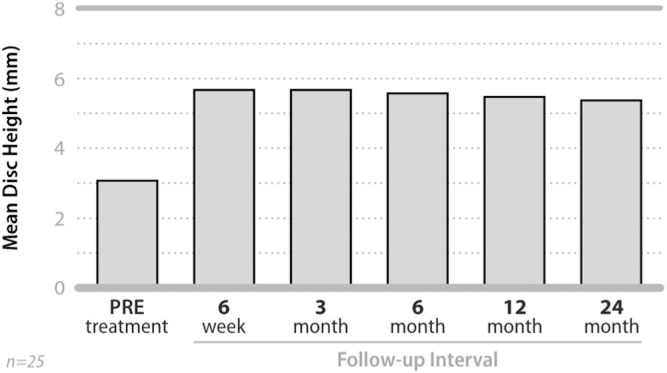
Conclusions: These findings indicate substantial clinical improvement for all function, pain, and quality of life outcomes in addition to maintenance of ROM and increase in disc height at the treated level(s). The findings also exhibit an acceptable safety profile, as indicated by the absence of serious adverse events and reoperations following arthroplasty with a next-generation artificial cervical disc replacement device.
Keywords: Cervical disc herniation; Cervical disc replacement; Cervical stenosis; M6-C artificial cervical disc.
Figures



References
-
- Albert TJ, Murrell SE. Surgical management of cervical radiculopathy. J Am Acad Orthop Surg. 1999;7:368–76. - PubMed
-
- Carette S, Fehlings MG. Clinical practice. Cervical radiculopathy. N Engl J Med. 2005;353:392–9. - PubMed
-
- Chesnut RM, Abitbol JJ, Garfin SR. Surgical management of cervical radiculopathy. Indication, techniques, and results. Orthop Clin North Am. 1992;23:461–74. - PubMed
-
- Hilibrand AS, Balasubramanian K, Eichenbaum M, et al. The effect of anterior cervical fusion on neck motion. Spine. 2006;31:1688–92. - PubMed
-
- Lopez-Espina CG, Amirouche F, Havalad V. Multilevel cervical fusion and its effect on disc degeneration and osteophyte formation. Spine. 2006;31:972–8. - PubMed
LinkOut - more resources
Full Text Sources