

Two-year clinical and radiographic success of minimally invasive lateral transpsoas approach for the treatment of degenerative lumbar conditions
- PMID: 25802648
- PMCID: PMC4365615
- DOI: 10.1016/j.esas.2010.03.005
Two-year clinical and radiographic success of minimally invasive lateral transpsoas approach for the treatment of degenerative lumbar conditions
Abstract
Background: The lateral transpsoas approach to interbody fusion is a less disruptive but direct-visualization approach for anterior/anterolateral fusion of the thoracolumbar spine. Several reports have detailed the technique, the safety of the approach, and the short term clinical benefits. However, no published studies to date have reported the long term clinical and radiographic success of the procedure.
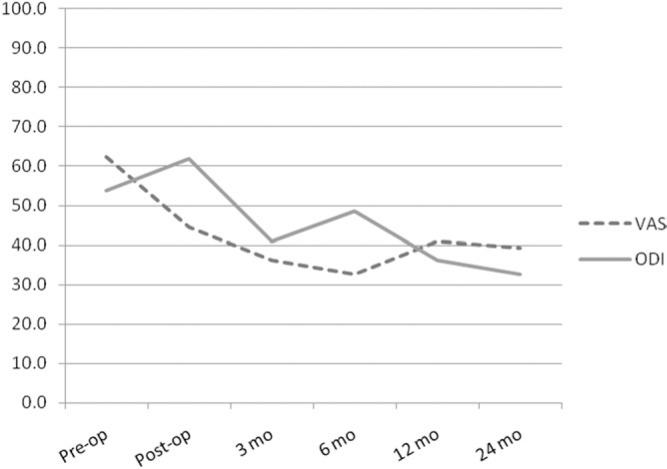
Materials and methods: The current study is a retrospective chart review of prospectively collected clinical and radiographic outcomes in 62 patients having undergone the Anterolateral transpsoas procedure at a single institution for anterior column stabilization as treatment for degenerative conditions, including degenerative disk disease, spondylolisthesis, scoliosis, and stenosis. Only patients who were a minimum of 2 years postoperative were included in this evaluation. Clinical outcomes measured included visual analog pain scales (VAS) and Oswestry disability index (ODI). Radiographic outcomes included identification of successful arthrodesis.
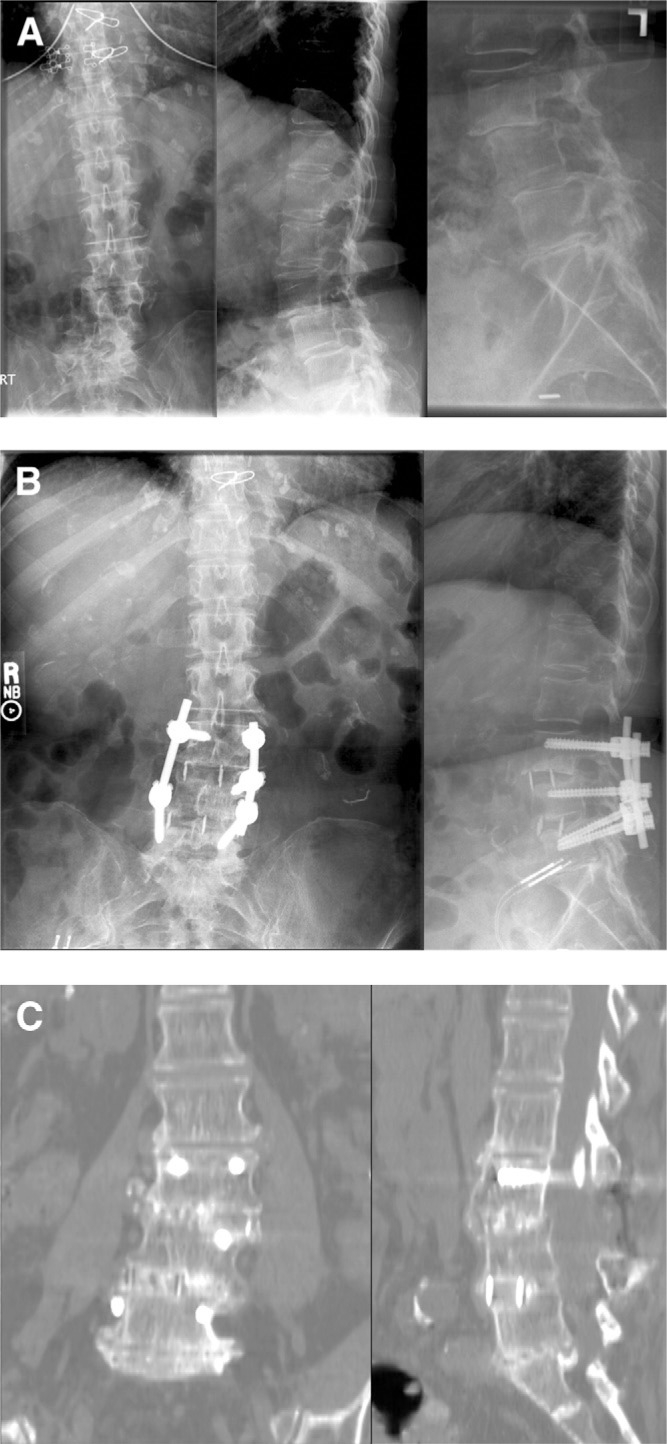
Results: Sixty-two patients were treated with lateral interbody fusion between 2003 and December 2006. Twenty-six patients (42%) were single-level, 13 (21%) 2-level, and 23 (37%) 3- or more levels. Forty-five (73%) included supplemental posterior pedicle fixation, 4 (6%) lateral fixation, and 13 (21%) were stand-alone. Pain scores (VAS) decreased significantly from preoperative to 2 years follow-up by 37% (P < .0001). Functional scores (ODI) decreased significantly by 39% from preoperative to 2 years follow-up (P < .0001). Clinical success by ODI-change definition was achieved in 71% of patients. Radiographic success was achieved in 91% of patients, with 1 patient with pseudarthrosis requiring posterior revision.
Conclusion: The lateral transpsoas approach is similar to a traditional anterior lumbar interbody fusion, in that access is obtained through a retroperitoneal, direct-visualization exposure, and a large implant can be placed in the interspace to achieve disk height and alignment correction. The 2 years plus clinical and radiographic success rates are similar to or better than those reported for traditional anterior and posterior approach procedures, which, coupled with significant short-term benefits of minimal morbidity, make the lateral approach a safe and effective treatment option for anterior/anterolateral lumbar fusions.
Keywords: Anterolateral; Lateral fusion; Lateral transpsoas; Minimally invasive.
Figures
References
-
- McAfee PC, DeVine JG, Chaput CD, et al. The indications for interbody fusion cages in the treatment of spondylolisthesis: analysis of 120 cases. Spine (Phila Pa 1976) 2005;30(6 Suppl):S60–5. - PubMed
-
- Resnick DK, Choudhri TF, Dailey AT, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 2: assessment of functional outcome. J Neurosurg Spine. 2005;2:639–46. - PubMed
-
- Brantigan JW, Steffee AD, Lewis ML, Quinn LM, Persenaire JM. Lumbar interbody fusion using the Brantigan I/F cage for posterior lumbar interbody fusion and the variable pedicle screw placement system: two-year results from a Food and Drug Administration investigational device exemption clinical trial. Spine (Phila Pa 1976) 2000;25:1437–46. - PubMed
-
- Fritzell P, Hagg O, Wessberg P, Nordwall A. 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: a multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine (Phila Pa 1976) 2001;26:2521–32. discussion 2532–2524. - PubMed
-
- Kuslich SD, Ulstrom CL, Griffith SL, Ahern JW, Dowdle JD. The Bagby and Kuslich method of lumbar interbody fusion. History, techniques, and 2-year follow-up results of a United States prospective, multicenter trial. Spine (Phila Pa 1976) 1998;23:1267–78. - PubMed
LinkOut - more resources
Full Text Sources