

Spatial Variation in the Healthy Human Lung Microbiome and the Adapted Island Model of Lung Biogeography
- PMID: 25803243
- PMCID: PMC4590020
- DOI: 10.1513/AnnalsATS.201501-029OC
Spatial Variation in the Healthy Human Lung Microbiome and the Adapted Island Model of Lung Biogeography
Abstract
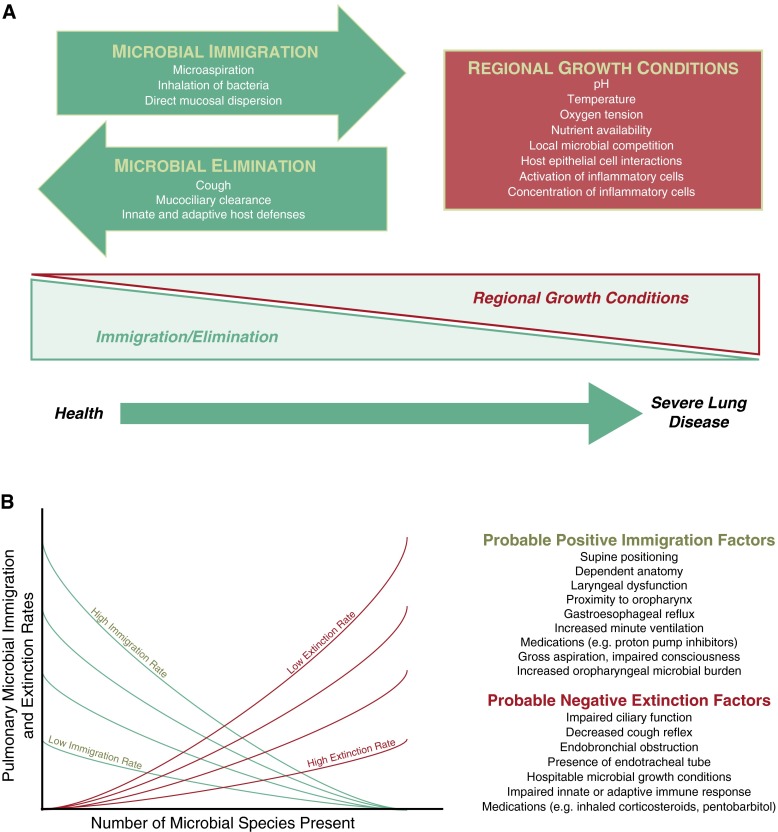
Rationale: The lung microbiome is spatially heterogeneous in advanced airway diseases, but whether it varies spatially in health is unknown. We postulated that the primary determinant of lung microbiome constitution in health is the balance of immigration and elimination of communities from the upper respiratory tract (URT; "adapted island model of lung biogeography"), rather than differences in regional bacterial growth conditions.
Objectives: To determine if the lung microbiome is spatially varied in healthy adults.
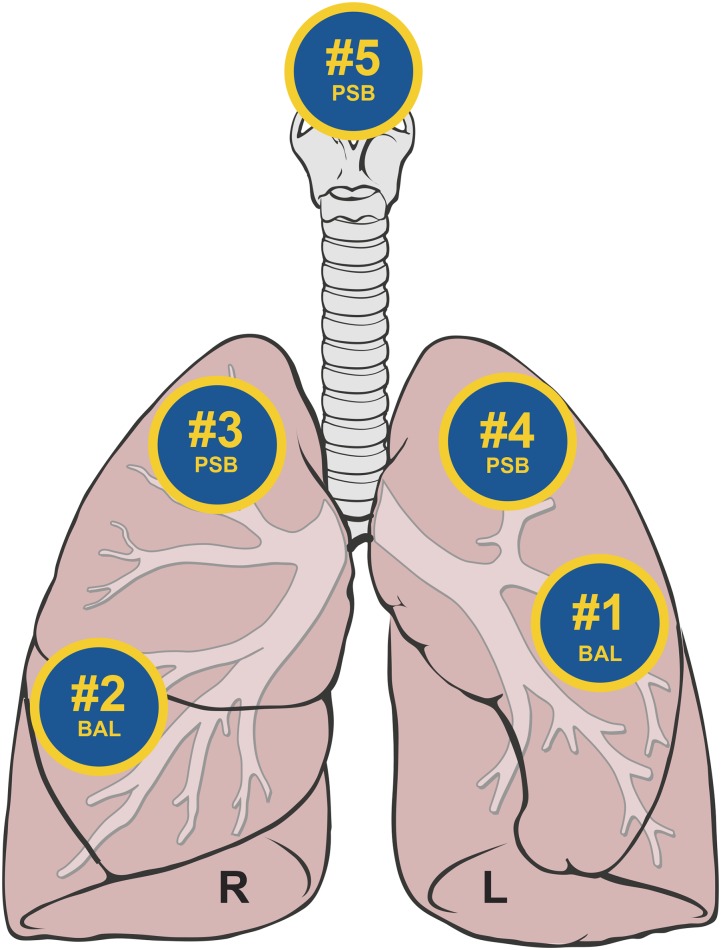
Methods: Bronchoscopy was performed on 15 healthy subjects. Specimens were sequentially collected in the lingula and right middle lobe (by bronchoalveolar lavage [BAL]), then in the right upper lobe, left upper lobe, and supraglottic space (by protected-specimen brush). Bacterial 16S ribosmal RNA-encoding genes were sequenced using MiSeq (Illumina, San Diego, CA).
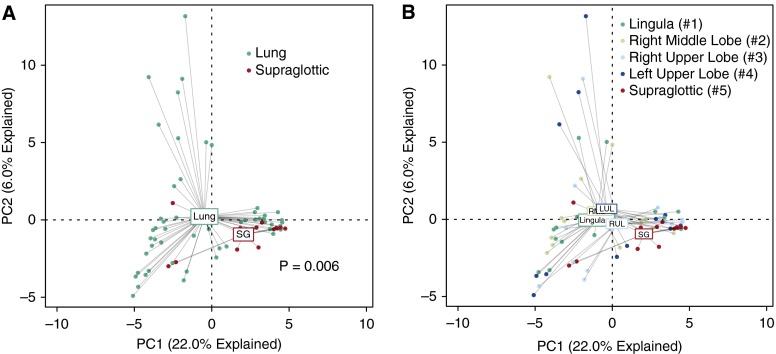
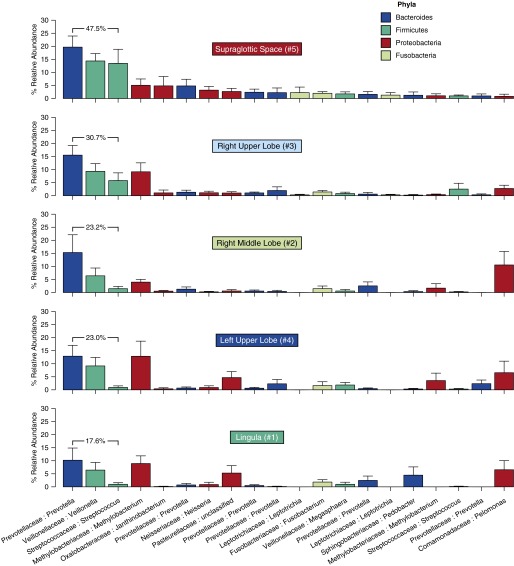
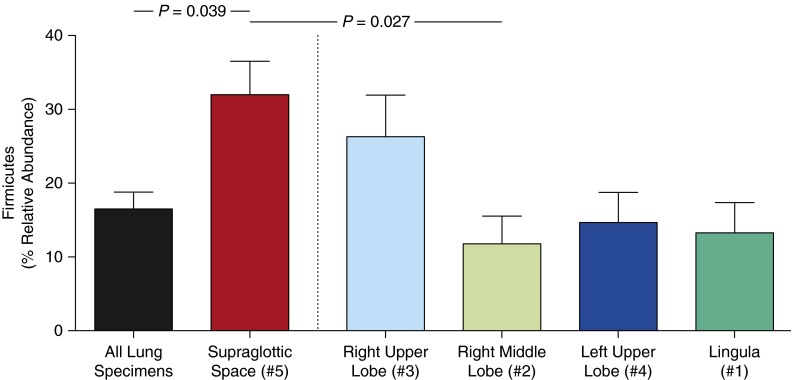
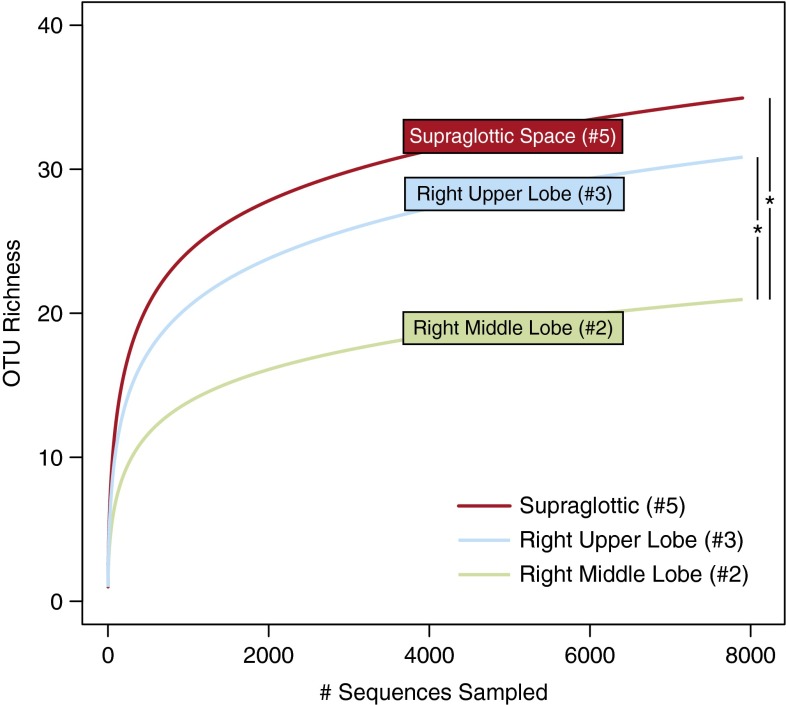
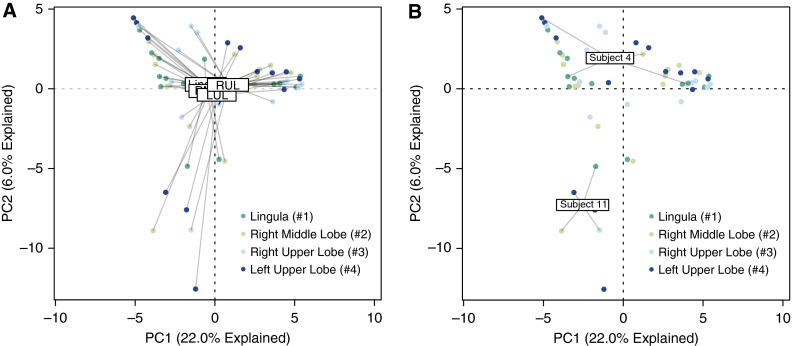
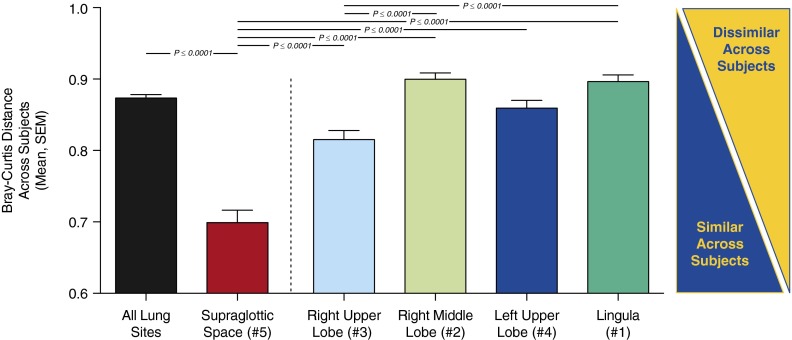
Measurements and main results: There were no significant differences between specimens collected by BAL and protected-specimen brush. Spatially separated intrapulmonary sites, when compared with each other, did not contain consistently distinct microbiota. On average, intrasubject variation was significantly less than intersubject variation (P = 0.00003). By multiple ecologic parameters (community richness, community composition, intersubject variability, and similarity to source community), right upper lobe microbiota more closely resembled those of the URT than did microbiota from more distal sites. As predicted by the adapted island model, community richness decreased with increasing distance from the source community of the URT (P < 0.05).
Conclusions: In healthy lungs, spatial variation in microbiota within an individual is significantly less than variation across individuals. The lung microbiome in health is more influenced by microbial immigration and elimination (the adapted island model) than by the effects of local growth conditions on bacterial reproduction rates, which are more determinant in advanced lung diseases. BAL of a single lung segment is an acceptable method of sampling the healthy lung microbiome. Clinical trial registered with www.clinicaltrials.gov (NCT02392182).
Keywords: 16S ribosomal DNA; bronchoscopy; lung; microbiome.
Figures
References
-
- Segal LN, Alekseyenko AV, Clemente JC, Kulkarni R, Wu B, Chen H, Berger KI, Goldring RM, Rom WN, Blaser MJ, et al. Enrichment of lung microbiome with supraglottic taxa is associated with increased pulmonary inflammation. Microbiome. 2013;1:19. [Published erratum appears in Microbiome 2:21.] - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
