

Evaluation of the influence of a pharmacist-led patient-centered medication therapy management and reconciliation service in collaboration with emergency department physicians
- PMID: 25803763
- PMCID: PMC10397596
- DOI: 10.18553/jmcp.2015.21.4.298
Evaluation of the influence of a pharmacist-led patient-centered medication therapy management and reconciliation service in collaboration with emergency department physicians
Abstract
Background: The implementation of the Patient Protection and Affordable Care Act is anticipated to increase the frequency of emergency department (ED) visits. Therefore, there is a critical need to improve the quality of care transitions among ED patients from ED to outpatient services.
Objective: To evaluate the effect of systematic implementation of a pharmacist-led patient-centered approach to medication therapy management and reconciliation service (MRS) in the ED on patient utilization of available health care services.
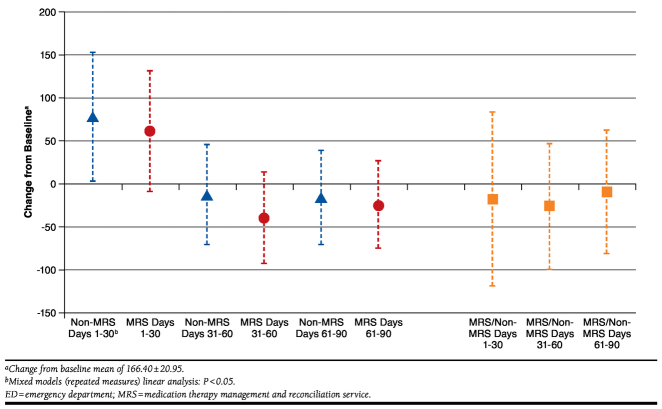
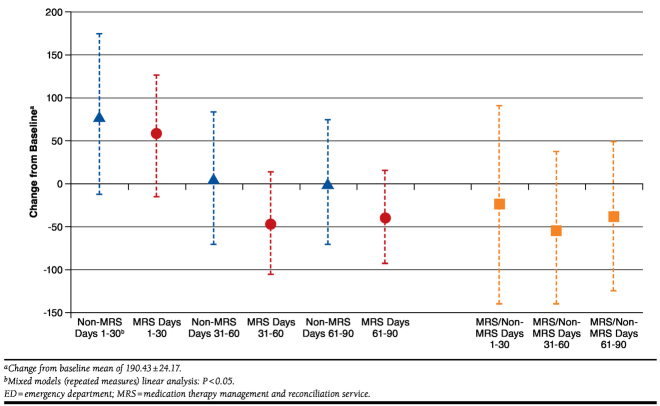
Methods: A single institution prospective randomized cohort study with 90-day postvisit observation randomized patients into 2 groups: (1) medication therapy management reconciliation service following a patient-centered approach (MRS) or (2) usual care provided by the institution (non-MRS). To align patient enrollment with availability of other primary care services, subjects were enrolled during weekday daytime hours. Data for the 90 days before and after the index ED visit were matched in all analyses. Generalized estimating equations evaluated any primary care (PC), urgent care (UC), and ED visits during the 90 days post-index ED visit, adjusted by age and sex and weighted by survival time. Generalized linear models evaluated the average number of ED visits during that period, adjusted by age and sex and weighted by survival time. Data were analyzed for all adult patients (ADLTS), aged ≥ 18 years, and the subpopulation taking 1 or more prescribed daily medication at the time of the index ED visit (ADLTS1+)-the patients expected to receive greatest benefit from an MRS program.
Results: ADLTS MRS patients were 1.9 more likely than non-MRS patients to visit their PC providers (mean difference 0.15, P less than 0.001). Similarly, ADLTS1+ MRS patients were 1.5 times more likely to visit their PC providers (mean difference 0.10, P = 0.026). Although ADLT MRS patients were less likely to visit the UC, this was not significant. However, ADLTS1+ MRS patients were significantly less likely than non-MRS patients (OR = 0.5, 95% CI = 0.3-0.9) to visit the UC. No significant difference was seen in ED visits.
Conclusions: The implementation of a patient-centered approach to medication therapy management and reconciliation improved the odds of patients visiting their PC providers, a positive first step in transitioning patients toward an appropriate use of PC services.
Conflict of interest statement
Research for this study was funded by Essentia Health Foundation. The authors declare no conflicts of interest.
Study concept and design were primarily contributed by Nkemdirim Okere, along with Renier and Tomsche. Data were collected and analysed by Nkemdirim Okere and Renier. The manuscript was primarily written by Nkemdirim Okere, along with Renier, and was revised equally by Nkemdirim Okere and Renier.
Figures
References
-
- Centers for Disease Control and Prevention. National Hospital Ambulatory Medical Care Survey: 2010 Emergency department summary. Available at: http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2010_ed_web_tables.pdf. Accessed January 19, 2015.
-
- McCaig LF, Burt CW.. National Hospital Ambulatory Medical Care Survey: 2002 emergency department summary. Adv Data. 2004;(340):1-34. - PubMed
-
- Smulowitz PB, O’Malley J, Yang X, Landon BE.. Increased use of the emergency department after health care reform in Massachusetts. Ann Emerg Med. 2014;64(2):107-15. - PubMed
-
- Coleman EA, Eilertsen TB, Kramer AM, Magid DJ, Beck A, Conner D.. Reducing emergency visits in older adults with chronic illness. A randomized, controlled trial of group visits. Eff Clin Pract. 2001;4(2):49-57. - PubMed
-
- Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc. 2003;51(4):549-55. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
