

Psychological therapies (remotely delivered) for the management of chronic and recurrent pain in children and adolescents
- PMID: 25803793
- PMCID: PMC4833498
- DOI: 10.1002/14651858.CD011118.pub2
Psychological therapies (remotely delivered) for the management of chronic and recurrent pain in children and adolescents
Update in
-
Psychological therapies (remotely delivered) for the management of chronic and recurrent pain in children and adolescents.Cochrane Database Syst Rev. 2019 Apr 2;4(4):CD011118. doi: 10.1002/14651858.CD011118.pub3. Cochrane Database Syst Rev. 2019. PMID: 30939227 Free PMC article.
Abstract
Background: Chronic pain is common during childhood and adolescence and is associated with negative outcomes such as increased severity of pain, reduced function (e.g. missing school), and low mood (e.g. high levels of depression and anxiety). Psychological therapies, traditionally delivered face-to-face with a therapist, are efficacious at reducing pain intensity and disability. However, new and innovative technology is being used to deliver these psychological therapies remotely, meaning barriers to access to treatment such as distance and cost can be removed or reduced. Therapies delivered with technological devices, such as the Internet, computer-based programmes, smartphone applications, or via the telephone, can be used to deliver treatment to children and adolescents with chronic pain.
Objectives: To determine the efficacy of psychological therapies delivered remotely compared to waiting-list, treatment-as-usual, or active control treatments, for the management of chronic pain in children and adolescents.
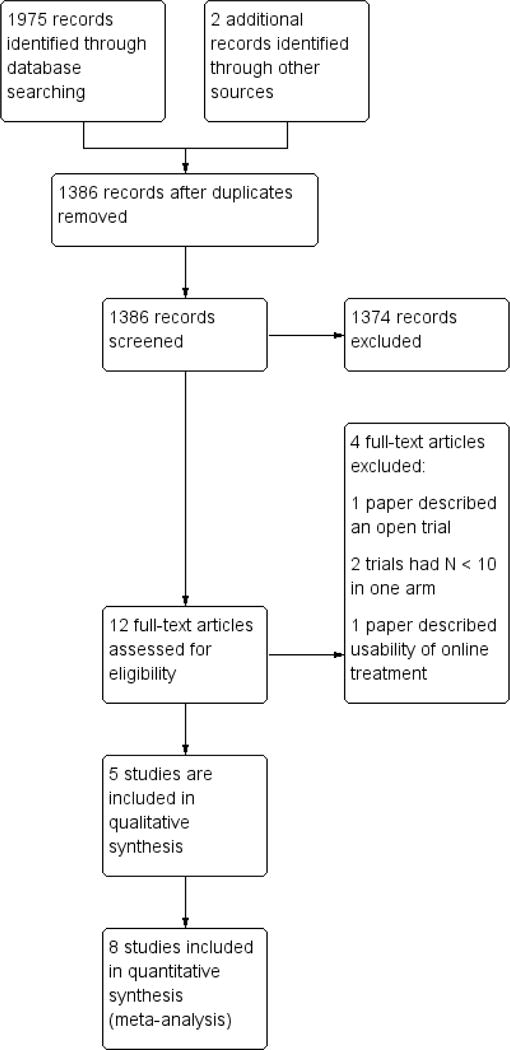
Search methods: We searched four databases (CENTRAL, MEDLINE, EMBASE, and PsycINFO) from inception to June 2014 for randomised controlled trials of remotely delivered psychological interventions for children and adolescents (0 to 18 years of age) with chronic pain. We searched for chronic pain conditions including, but not exclusive to, headache, recurrent abdominal pain, musculoskeletal pain, and neuropathic pain. We also searched online trial registries for potential trials. A citation and reference search for all included studies was conducted.
Selection criteria: All included studies were randomised controlled trials that investigated the efficacy of a psychological therapy delivered remotely via the Internet, smartphone device, computer-based programme, audiotapes, or over the phone in comparison to an active, treatment-as-usual, or waiting-list control. We considered blended treatments, which used a combination of technology and face-to-face interaction. We excluded interventions solely delivered face-to-face between therapist and patient from this review. Children and adolescents (0 to 18 years of age) with a primary chronic pain condition were the target of the interventions. Each comparator arm, at each extraction point had to include 10 or more participants.
Data collection and analysis: For the analyses, we combined all psychological therapies. We split pain conditions into headache and mixed (non-headache) pain and analysed them separately. Pain, disability, depression, anxiety, and adverse events were extracted as primary outcomes. We also extracted satisfaction with treatment as a secondary outcome. We considered outcomes at two time points: first immediately following the end of treatment (known as 'post-treatment'), and second, any follow-up time point post-treatment between 3 and 12 months (known as 'follow-up'). We assessed all included studies for risk of bias.
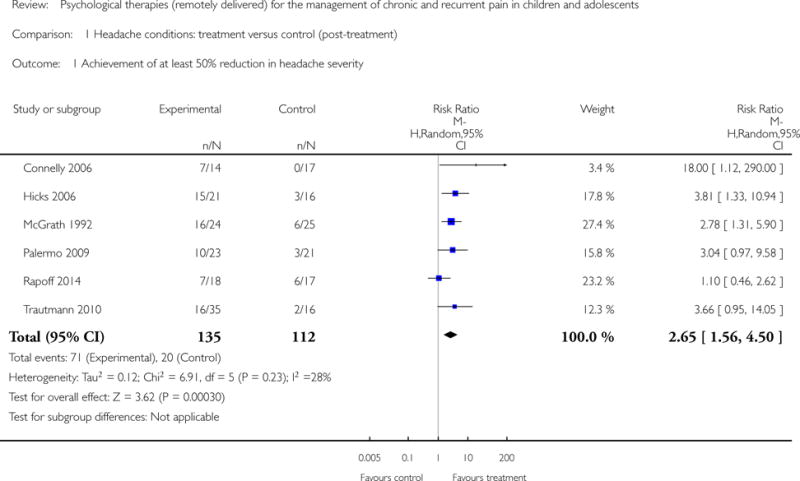
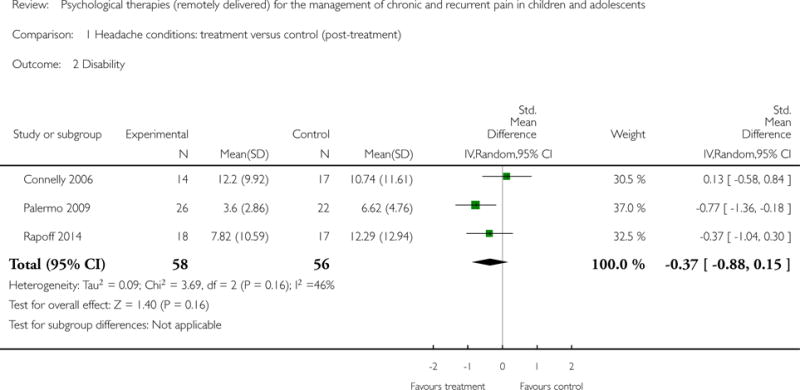
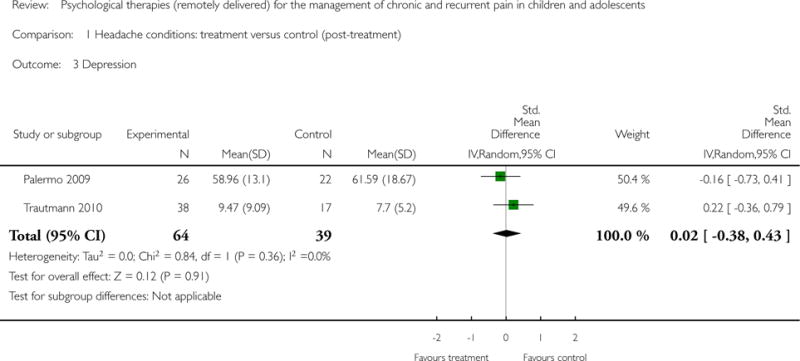
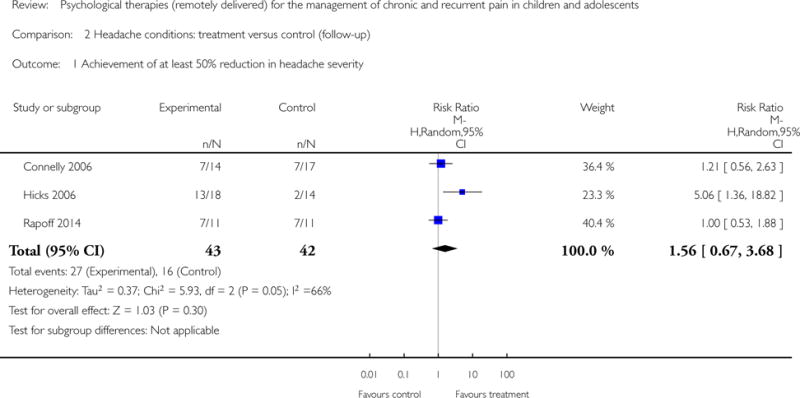
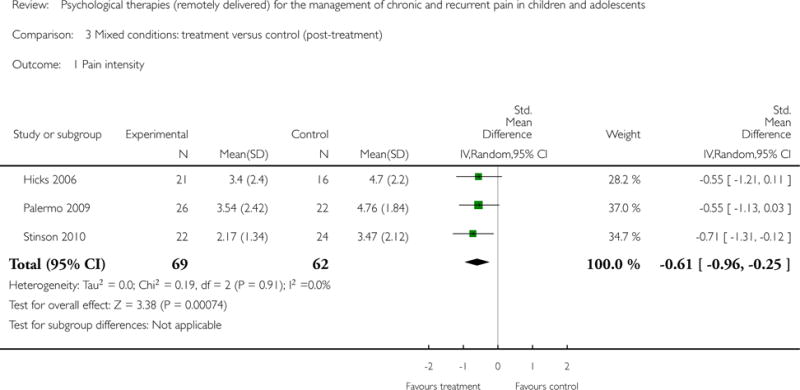
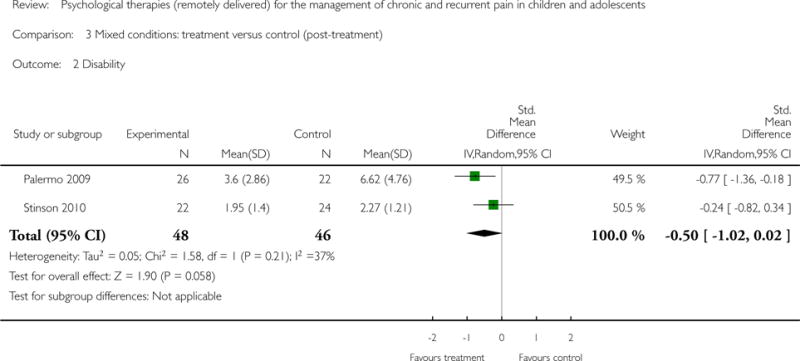
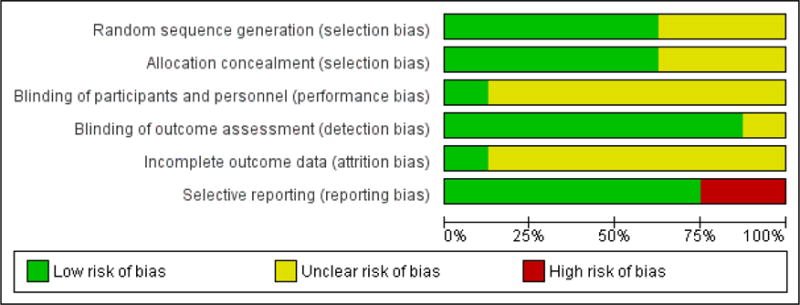
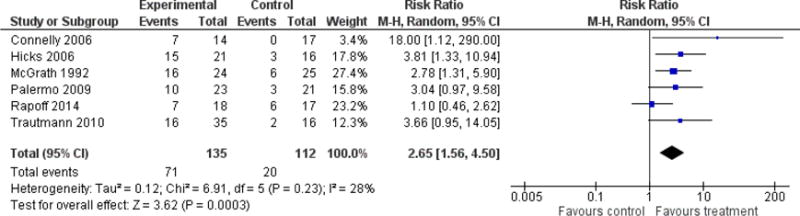
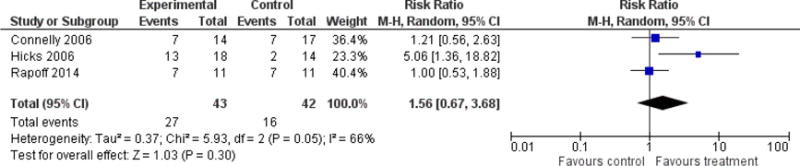
Main results: Eight studies (N = 371) that delivered treatment remotely were identified from our search; five studies investigated children with headache conditions, one study was with children with juvenile idiopathic arthritis, and two studies included mixed samples of children with headache and mixed (i.e. recurrent abdominal pain, musculoskeletal pain) chronic pain conditions. The average age of children receiving treatment was 12.57 years.For headache pain conditions, we found one beneficial effect of remotely delivered psychological therapy. Headache severity was reduced post-treatment (risk ratio (RR) = 2.65, 95% confidence interval (CI) 1.56 to 4.50, z = 3.62,p < 0.01, number needed to treat to benefit (NNTB) = 2.88). For mixed pain conditions, we found only one beneficial effect: psychological therapies reduced pain intensity post-treatment (standardised mean difference (SMD) = -0.61, 95% CI -0.96 to -0.25, z = 3.38, p < 0.01). No effects were found for reducing pain at follow-up in either analysis. For headache and mixed conditions, there were no beneficial effects of psychological therapies delivered remotely for disability post-treatment and a lack of data at follow-up meant no analyses could be run. Only one analysis could be conducted for depression outcomes. We found no beneficial effect of psychological therapies in reducing depression post-treatment for headache conditions. Only one study presented data in children with mixed pain conditions for depressive outcomes and no data were available for either condition at follow-up. Only one study presented anxiety data post-treatment and no studies reported follow-up data, therefore no analyses could be run. Further, there were no data available for adverse events, meaning that we are unsure whether psychological therapies are harmful to children who receive them. Satisfaction with treatment is described qualitatively.'Risk of bias' assessments were low or unclear. We judged selection, detection, and reporting biases to be mostly low risk for included studies. However, judgements made on performance and attrition biases were mostly unclear.
Authors' conclusions: Psychological therapies delivered remotely, primarily via the Internet, confer benefit in reducing the intensity or severity of pain after treatment across conditions. There is considerable uncertainty around these estimates of effect and only eight studies with 371 children contribute to the conclusions. Future studies are likely to change the conclusions reported here. All included trials used either behavioural or cognitive behavioural therapies for children with chronic pain, therefore we cannot generalise our findings to other therapies. However, satisfaction with these treatments was generally positive. Larger trials are needed to increase our confidence in all conclusions regarding the efficacy of remotely delivered psychological therapies. Implications for practice and research are discussed.
Conflict of interest statement
EF, EL, TP, and CE have no relevant declarations of interest.
For transparency we declare that we have received research support from charity, government, and industry sources at various times, but none relate to this review.
Figures

References
References to studies included in this review
-
- Connelly M, Rapoff MA, Thompson N, Connelly W. Headstrong: A pilot study of a CD-ROM intervention for recurrent pediatric headache. Journal of Pediatric Psychology. 2006;31:737–47. - PubMed
-
- Hicks CL, von Baeyer CL, McGrath PJ. Online psychological treatment for pediatric recurrent pain: a randomized evaluation. Journal of Pediatric Psychology. 2006;31:724–36. - PubMed
-
- McGrath PJ, Humphreys P, Keene D, Goodman JT, Lascelles MA, Cunningham J, et al. The efficacy and efficiency of a self-administered treatment for adolescent migraine. Pain. 1992;49:321–4. - PubMed
References to studies excluded from this review
-
- Bonnert M, Ljótsson B, Hedman E, Andersson J, Arnell H, Benninga M, et al. Internet-delivered cognitive behavior therapy for adolescents with functional gastrointestinal disorders – an open trial. Internet Interventions. in press.
-
- Merlijn VPBM, Hunfeld JAM, Van Der Wouden JC, Hazebroek-Kampschreur AAJM, Van Suijlekom-Smit LWA, Koes BW, et al. A cognitive-behavioural program for adolescents with chronic pain – a pilot study. Patient Education and Counseling. 2005;59(2):126–34. - PubMed
-
- Trautmann E, Kroner-Herwig Internet-based self-help training for children and adolescents with recurrent headache: a pilot study. Behavioural and Cognitive Psychotherapy. 2008;36(2):241–5.
Additional references
-
- Australian Bureau of Statistics. Use of Information Technology. www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/1301.0~2012~Main%20... (accessed October 2013)
-
- Andersson G, Ljótsson B, Weise C. Internet-delivered treatment to promote health. Current Opinion in Psychiatry. 2011;24(2):168–72. - PubMed
-
- Andrasik F, Powers SW, McGrath PJ. Methodological considerations in research with special populations: children and adolescents. Headache. 2005;45:520–5. - PubMed
-
- Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. Journal of Clinical Epidemiology. 2011;64(4):401–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical