Saskatchewan movement disorders program
- PMID: 25804247
- PMCID: PMC4416358
- DOI: 10.1017/cjn.2015.13
Saskatchewan movement disorders program
Abstract
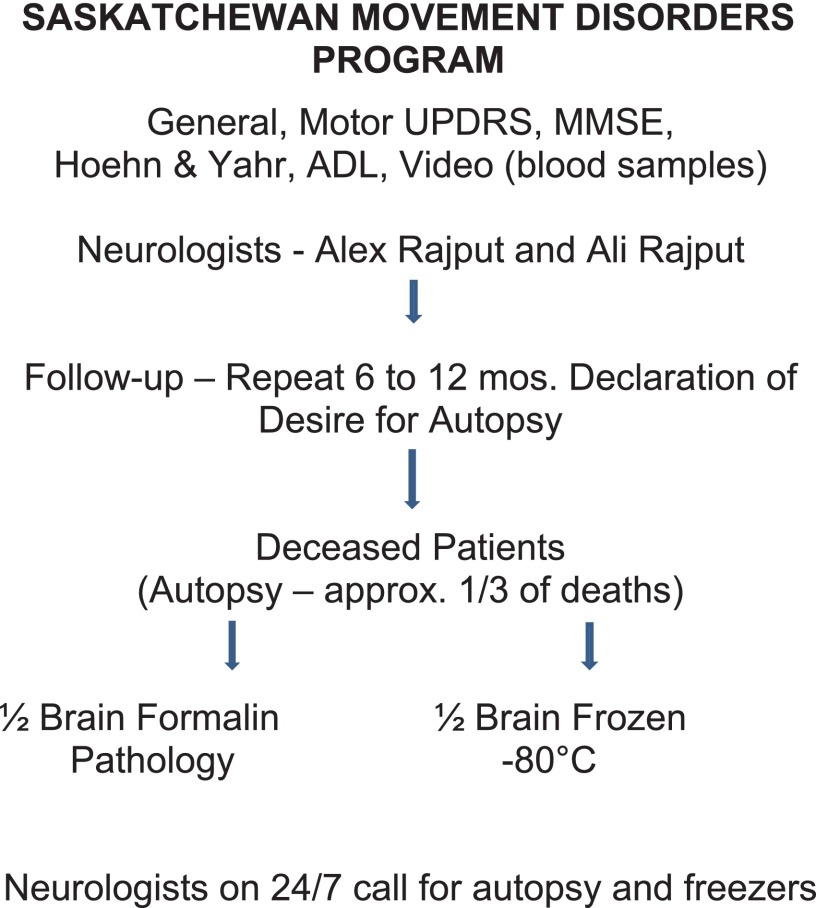
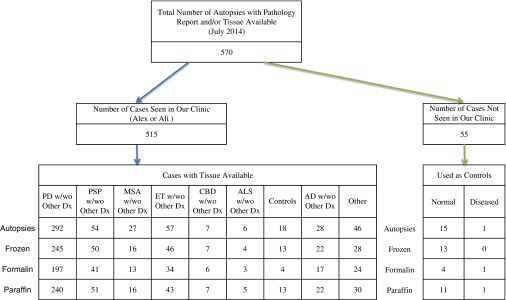
We review the Saskatchewan Movement Disorders Program, which started in 1968 and has had the dual goals of patient care and research. The clinics are structured to collect research-worthy data including videos, longitudinal follow-up, and autopsy studies of patients seen in the clinics. At every clinic visit, the patient is evaluated by one or both authors. A total of 25% to 30% of the deceased come to autopsy. Frozen half-brain and formalin-fixed remnants from autopsy are preserved in our laboratories. Patients not seen in our clinic are not included in research, which makes it different from brain banks. So far, 515 cases have come to autopsy. So far, there have been 17 collaborating scientific teams from Canada, the United States, Europe, and Japan. The collaborators are not charged for access to our resources. This program offers a unique opportunity to study multiple aspects of movement disorder patients seen in clinical practice.
Movement Disorders Program de la Saskatchewan. Nous avons revu le Movement Disorders Program de la Saskatchewan établi en 1968. Son but est double, soit les soins aux patients et la recherche. Les cliniques sont structurées de telle sorte que des données de qualité soient générées à des fins de recherche, incluant des vidéos, sur le suivi à long terme et l’autopsie de patients suivis à la clinique. À chaque visite à la clinique, le patient est évalué par l’un des auteurs ou par les deux. Une autopsie est effectuée chez 25% à 30% des patients qui décèdent. Des demi-cerveaux congelés provenant d’autopsies et des tissus conservés dans la formaline sont également conservés dans nos laboratoires. Les patients qui ne sont pas suivis à notre clinique ne sont pas inclus dans notre recherche, contrairement aux banques de cerveaux. À ce jour, 515 autopsies ont été réalisées et 17 équipes de recherche du Canada, des États-Unis, d’Europe et du Japon ont collaboré avec nous. Aucun frais n’est exigé des collaborateurs pour avoir accés à nos ressources. Ce programme offre une opportunité unique d’étudier les multiples aspects des troubles du mouvement rencontrés en pratique clinique.
Keywords: Parkinson disease.
Figures

References
-
- Ehringer H, Hornykiewicz O Distribution of noradrenaline and dopamine (3-hydroxytyramine) in human brain: their behaviour in extrapyramidal system diseases. Klin Wochenschr. 1960;38:1236-1239. - PubMed
-
- Birkmayer W, Hornykiewicz O The effect of L-3,4-dihydroxyphenylalanine (=L-DOPA) on akinesia in Parkinsonism. Wiener Klinische Wochenschrift. 1961;73:787-788. - PubMed
-
- Cotzias GC, Van Woert MH, Schiffer LM Aromatic amino acids and modification of Parkinsonism. N Engl J Med. 1967;276:374-379. - PubMed
-
- Rajput AH, Jamieson H, Hirsh S Specificity of tremorilytic effects of alcohol and propranolol. Clin Res. 1973;21:1018.
-
- Rajput AH, Jamieson H, Hirsch S, Quraishi A Relative efficacy of alcohol and propranolol in action tremor. Can J Neurol Sci. 1975;2:31-35. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical