

Augmentation of cardiac sympathetic tone by percutaneous low-level stellate ganglion stimulation in humans: a feasibility study
- PMID: 25804262
- PMCID: PMC4393162
- DOI: 10.14814/phy2.12328
Augmentation of cardiac sympathetic tone by percutaneous low-level stellate ganglion stimulation in humans: a feasibility study
Abstract
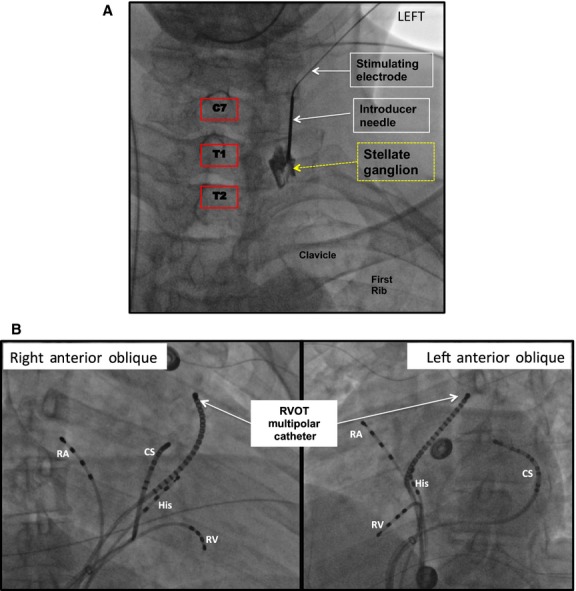
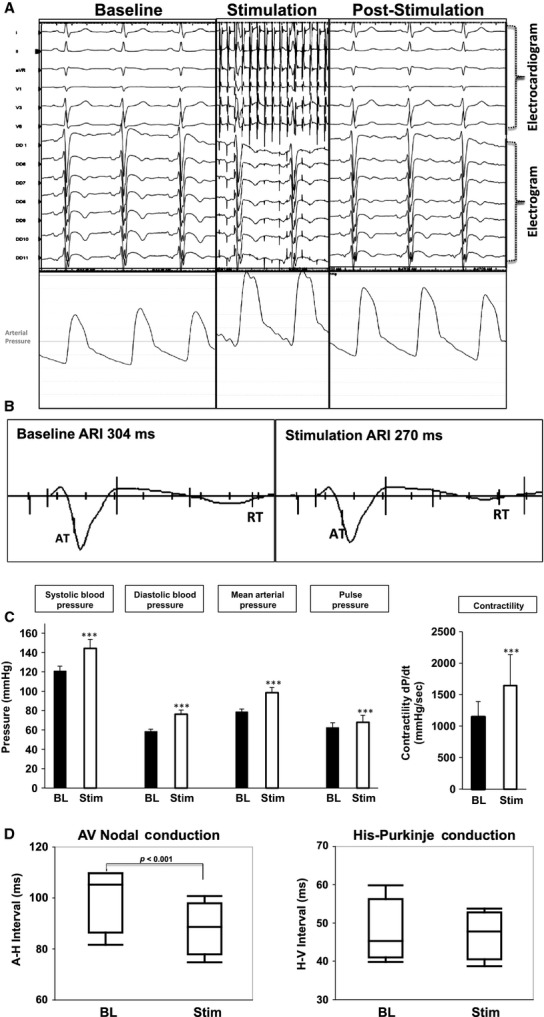
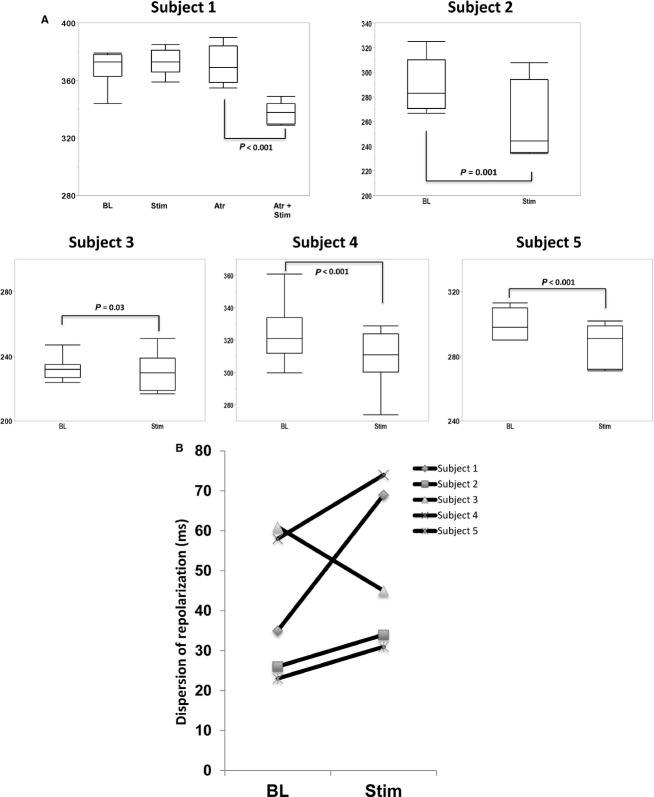
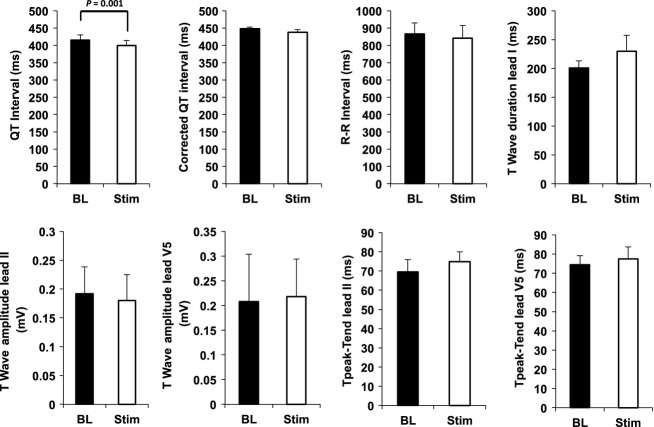
Modulation of human cardiac mechanical and electrophysiologic function by direct stellate ganglion stimulation has not been performed. Our aim was to assess the effect of low-level left stellate ganglion (LSG) stimulation (SGS) on arrhythmias, hemodynamic, and cardiac electrophysiological indices. Patients undergoing ablation procedures for arrhythmias were recruited for SGS. A stimulating electrode was placed next to the LSG under fluoroscopy and ultrasound imaging; and SGS (5-10 Hz, 10-20 mA) was performed. We measured hemodynamic, intracardiac and ECG parameters, and activation recovery intervals (ARIs) (surrogate for action potential duration) from a duodecapolar catheter in the right ventricular outflow tract. Five patients underwent SGS (3 males, 45 ± 20 years). Stimulating catheter placement was successful, and without complication in all patients. SGS did not change heart rate, but increased mean arterial blood pressure (78 ± 3 mmHg to 98 ± 5 mmHg, P < 0.001) and dP/dt max (1148 ± 244 mmHg/sec to 1645 ± 493 mmHg/sec, P = 0.03). SGS shortened mean ARI from 304 ± 23 msec to 283 ± 17 msec (P < 0.001), although one patient required parasympathetic blockade. Dispersion of repolarization (DOR) increased in four patients and decreased in one, consistent with animal models. QT interval, T-wave duration and amplitude at baseline and with SGS were 415 ± 15 msec versus 399 ± 15 msec (P < 0.001); 201 ± 12 msec versus 230 ± 28 msec; and 0.2 ± 0.09 mV versus 0.22 ± 0.08 mV, respectively. At the level of SGS performed, no increase in arrhythmias was seen. Percutaneous low-level SGS shortens ARI in the RVOT, and increases blood pressure and LV contractility. These observations demonstrate feasibility of percutaneous SGS in humans.
Keywords: Activation recovery interval; arrhythmias; stellate ganglion; sympathetic stimulation.
© 2015 The Authors. Physiological Reports published by Wiley Periodicals, Inc. on behalf of the American Physiological Society and The Physiological Society.
Figures
References
-
- Abdi S, Zhou Y, Patel N, Saini B. Nelson J. A new and easy technique to block the stellate ganglion. Pain Physician. 2004;7:327–331. - PubMed
-
- Abildskov JA. Adrenergic effects of the QT interval of the electrocardiogram. Am. Heart J. 1976;92:210–216. - PubMed
-
- Ackerman WE. Zhang JM. Efficacy of stellate ganglion blockade for the management of type 1 complex regional pain syndrome. South. Med. J. 2006;99:1084–1088. - PubMed
-
- Ajijola OA, Ramirez RJ, Laks MM, Zhou W, Mahajan A. Shivkumar K. ST segment shortening without QT interval shortening is a unique and novel marker of asymmetric cardiac sympathetic activation. Circulation. 2011;124:14010.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
