

Psychological treatments for early psychosis can be beneficial or harmful, depending on the therapeutic alliance: an instrumental variable analysis
- PMID: 25805118
- PMCID: PMC4501302
- DOI: 10.1017/S003329171500032X
Psychological treatments for early psychosis can be beneficial or harmful, depending on the therapeutic alliance: an instrumental variable analysis
Abstract
Background: The quality of the therapeutic alliance (TA) has been invoked to explain the equal effectiveness of different psychotherapies, but prior research is correlational, and does not address the possibility that individuals who form good alliances may have good outcomes without therapy.
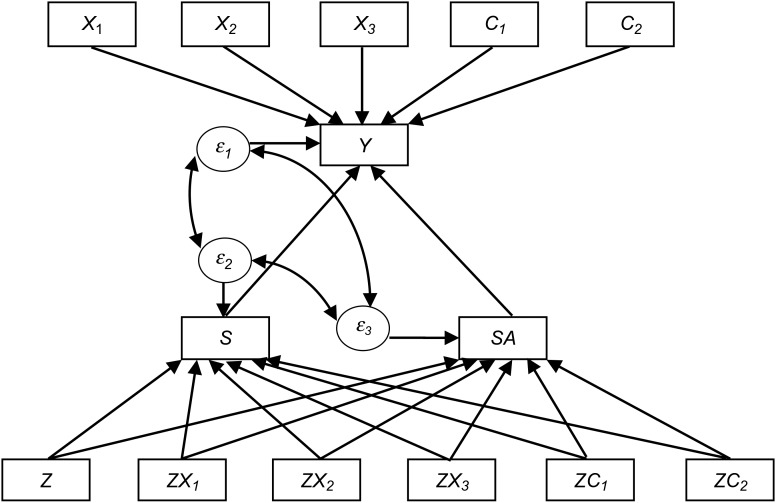
Method: We evaluated the causal effect of TA using instrumental variable (structural equation) modelling on data from a three-arm, randomized controlled trial of 308 people in an acute first or second episode of a non-affective psychosis. The trial compared cognitive behavioural therapy (CBT) over 6 weeks plus routine care (RC) v. supportive counselling (SC) plus RC v. RC alone. We examined the effect of TA, as measured by the client-rated CALPAS, on the primary trial 18-month outcome of symptom severity (PANSS), which was assessed blind to treatment allocation.
Results: Both adjunctive CBT and SC improved 18-month outcomes, compared to RC. We showed that, for both psychological treatments, improving TA improves symptomatic outcome. With a good TA, attending more sessions causes a significantly better outcome on PANSS total score [effect size -2.91, 95% confidence interval (CI) -0.90 to -4.91]. With a poor TA, attending more sessions is detrimental (effect size +7.74, 95% CI +1.03 to +14.45).
Conclusions: This is the first ever demonstration that TA has a causal effect on symptomatic outcome of a psychological treatment, and that poor TA is actively detrimental. These effects may extend to other therapeutic modalities and disorders.
Keywords: Cognitive therapy; counselling; first episode; psychosis; therapeutic alliance.
Figures
References
-
- Cuijpers P, van Straten A, Andersson G, van Oppen P (2008). Psychotherapy for depression in adults: a meta-analysis of comparative outcome studies. Journal of Consulting and Clinical Psychology 76, 909–922. - PubMed
-
- Davis LW, Lysaker PH (2007). Therapeutic alliance and improvements in work performance over time in patients with schizophrenia. Journal of Nervous and Mental Disorders 195, 353–357. - PubMed
-
- Day JC, Bentall RP, Roberts C, Randall F, Rogers A, Cattell D, Healy D, Rae P, Power C (2005). Attitudes toward antipsychotic medication: the impact of clinical variables and relationships with health professionals. Archives of General Psychiatry 62, 717–724. - PubMed
-
- Dunn G, Bentall R (2007). Modelling treatment-effect heterogeneity in randomized controlled trials of complex interventions (psychological treatments). Statistics in Medicine 26, 4719–4745. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
