

An abdominal computed tomography may be safe in selected hypotensive trauma patients with positive Focused Assessment with Sonography in Trauma examination
- PMID: 25805456
- PMCID: PMC4822493
- DOI: 10.1016/j.amjsurg.2015.01.005
An abdominal computed tomography may be safe in selected hypotensive trauma patients with positive Focused Assessment with Sonography in Trauma examination
Abstract
Background: Positive Focused Assessment with Sonography in Trauma examination and hypotension often indicate urgent surgery. An abdomen/pelvis computed tomography (apCT) may allow less invasive management but the delay may be associated with adverse outcomes.
Methods: Patients in the Prospective Observational Multicenter Major Trauma Transfusion study with hypotension and a positive Focused Assessment with Sonography in Trauma (HF+) examination who underwent a CT (apCT+) were compared with those who did not.
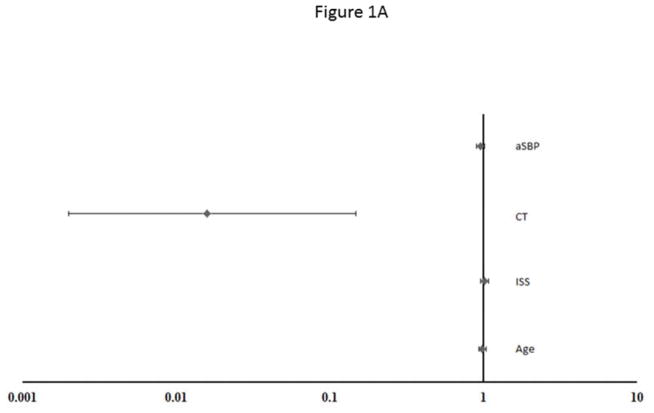
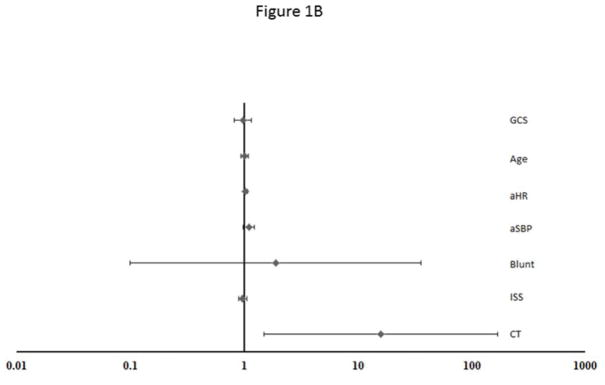
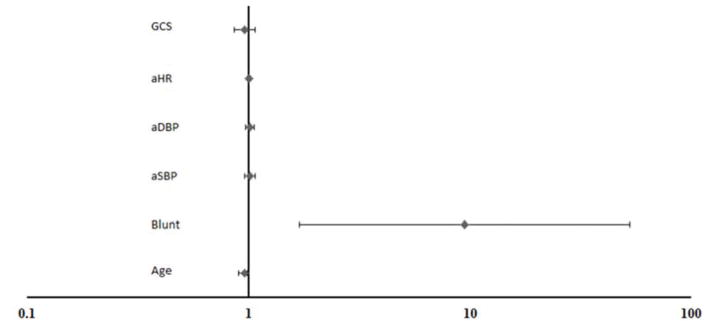
Results: Of the 92 HF+ identified, 32 (35%) underwent apCT during initial evaluation and apCT was associated with decreased odds of an emergency operation (odds ratio .11, 95% confidence interval .001 to .116) and increased odds of angiographic intervention (odds ratio 14.3, 95% confidence interval 1.5 to 135). There was no significant difference in 30-day mortality or need for dialysis.
Conclusions: An apCT in HF+ patients is associated with reduced odds of emergency surgery, but not mortality. Select HF+ patients can safely undergo apCT to obtain clinically useful information.
Keywords: Computed tomography scan; FAST examination; Trauma.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- MacLeod JB, Lynn M, McKenney MG, Cohn SM, Murtha M. Early coagulopathy predicts mortality in trauma. Journal of Trauma-Injury Infection & Critical Care. 2003;55(1):39–44. - PubMed
-
- Stengel D, Bauwens K, Sehouli J, et al. Systematic review and meta-analysis of emergency ultrasonography for blunt abdominal trauma. Br J Surg. 2001;88(7):901–912. - PubMed
-
- Bardenheuer M, Obertacke U, Waydhas C, Nast-Kolb D. Epidemiology of the severely injured patient. A prospective assessment of preclinical and clinical management. AG polytrauma of DGU. Unfallchirurg. 2000;103(5):355–363. - PubMed
-
- Stengel D, Bauwens K, Rademacher G, Ekkernkamp A, Guthoff C. Emergency ultrasound-based algorithms for diagnosing blunt abdominal trauma. Cochrane Database Syst Rev. 2013;7:CD004446. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
