

A Randomized Controlled Trial Comparing Two Multimodal Analgesic Techniques in Patients Predicted to Have Severe Pain After Cesarean Delivery
- PMID: 25806400
- PMCID: PMC5223090
- DOI: 10.1213/ANE.0000000000000695
A Randomized Controlled Trial Comparing Two Multimodal Analgesic Techniques in Patients Predicted to Have Severe Pain After Cesarean Delivery
Abstract
Background: Improved pain control after cesarean delivery remains a challenging objective. Poorly treated acute pain following delivery is associated with an increased risk of chronic pain and depression. This study was conducted to determine whether the addition of systemic acetaminophen and an increased dose of intrathecal morphine would further reduce acute pain. The primary outcome was pain intensity with movement at 24 hours postoperatively. Secondary measures included persistent pain and depression at 8 weeks.
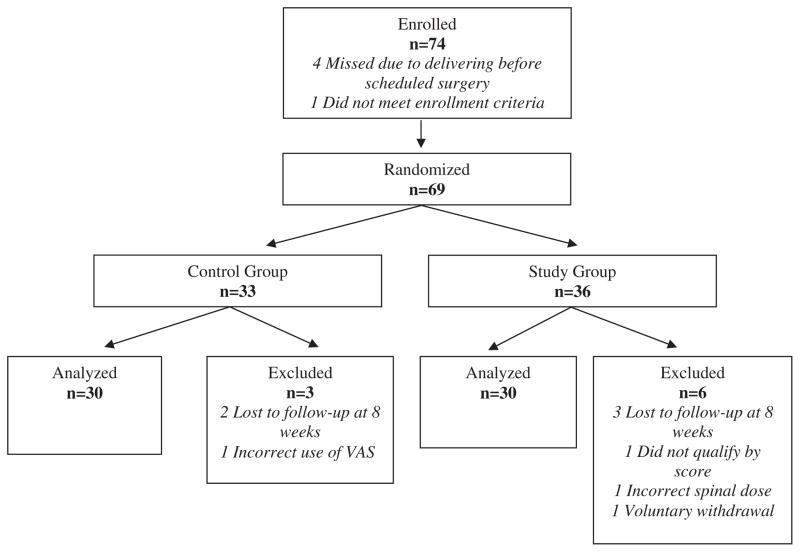
Methods: Seventy-four parturients scheduled for elective cesarean delivery under spinal anesthesia that were predicted to be above the 80th percentile for evoked pain intensity based on a 3-item preoperative screening questionnaire were enrolled. Patients in the intervention group received 300 mcg spinal morphine and 1 gram acetaminophen every 6 hours for 24 hours postoperatively. Patients in the control group received 150 mcg spinal morphine and placebo tablets. All patients received scheduled ibuprofen by mouth and IV morphine patient-controlled analgesia. At 24 hours, patients rated their pain intensity with movement, at rest, on average, and worst score using a visual analog scale for pain (100-mm unmarked line). The presence of persistent pain and depression was assessed at 8 weeks using the Edinburgh postpartum depression survey.
Results: Providing a higher dose of spinal morphine combined with systemic acetaminophen to patients predicted to be at high risk for severe post-cesarean delivery pain significantly reduced evoked pain scores with movement at 24 hours (mean ± SD: 46 ± 25 mm in control group versus 31 ±17 mm in intervention group, P = 0.009; 95% confidence interval for the difference between means: 4 mm, 26 mm). There was no difference in the incidence of persistent pain (13% (4/30) in control group versus 10% (3/30) in intervention group, P > 0.99), or depression at 8 weeks postoperatively (10% (3/30) in control group versus 13% (4/30) in intervention group, P > 0.99).
Conclusions: Adding a higher dose of intrathecal morphine and oral acetaminophen to a multimodal pain regimen in patients predicted to be at risk for high acute postpartum pain after cesarean delivery results in a significant reduction of acute postoperative pain scores at 24 hours.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Nikolajsen L, Sørensen HC, Jensen TS, Kehlet H. Chronic pain following Caesarean section. Acta Anaesthesiol Scand. 2004;48:111–6. - PubMed
-
- Kainu JP, Sarvela J, Tiippana E, Halmesmäki E, Korttila KT. Persistent pain after caesarean section and vaginal birth: a cohort study. Int J Obstet Anesth. 2010;19:4–9. - PubMed
-
- Pan PH, Coghill R, Houle TT, Seid MH, Lindel WM, Parker RL, Washburn SA, Harris L, Eisenach JC. Multifactorial preoperative predictors for postcesarean section pain and analgesic requirement. Anesthesiology. 2006;104:417–25. - PubMed
-
- Granot M, Lowenstein L, Yarnitsky D, Tamir A, Zimmer EZ. Postcesarean section pain prediction by preoperative experimental pain assessment. Anesthesiology. 2003;98:1422–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
