

Empiric treatment of neonatal sepsis in developing countries
- PMID: 25806843
- PMCID: PMC6858865
- DOI: 10.1097/INF.0000000000000692
Empiric treatment of neonatal sepsis in developing countries
Abstract
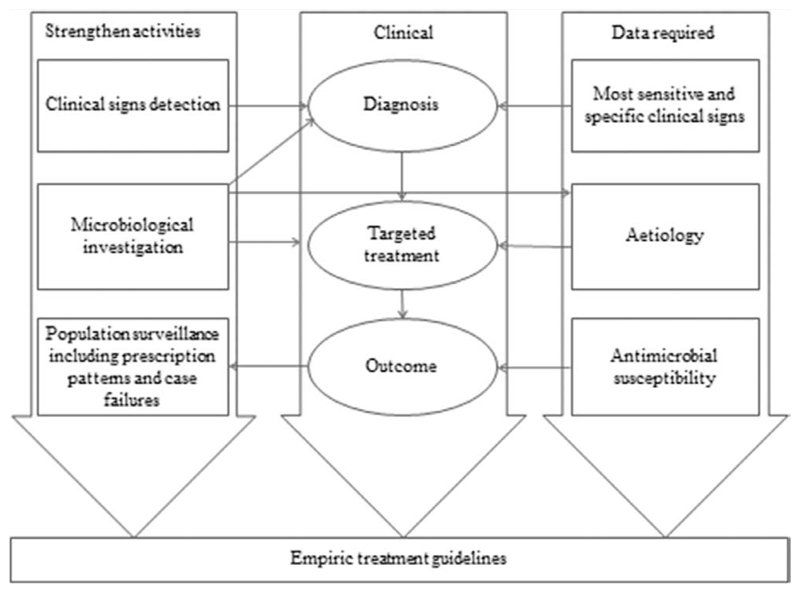
Infections are among the leading causes of neonatal mortality, and about 75% of the burden occurs in developing countries. Diagnosis of neonatal sepsis in these countries is dependent on the recognition of a set of nonspecific clinical signs that maximize sensitivity because staff making initial assessments may not have specialist pediatric training. Accurate diagnosis is usually limited by the unavailability of reliable microbiological investigation. The World Health Organization recommends ampicillin (or penicillin; cloxacillin if staphylococcal infection is suspected) plus gentamicin for empiric treatment of neonates with suspected clinical sepsis or meningitis. However, there is a lack of comprehensive data on the causes of infection and antimicrobial susceptibility in developing countries to support these recommendations, especially in rural settings. Bacterial pathogens (predominantly Gram negative) with reduced susceptibility to empiric medication have been reported, with variations both between and within regions. Nosocomial infections with resistant organisms and high case fatality challenge the first-line use of cephalosporins. Improving local surveillance data using standardized antimicrobial susceptibility testing methods and validation of diagnostic algorithms against microbial findings are essential. Standardized reporting of treatment outcomes is required to evaluate practice, provide guidance on second-line regimes and for studies of new approaches, such as simplified community-based regimens, and to determine the appropriate duration of empiric treatment for apparently low-risk neonates with early resolution of clinical signs, or where available, negative blood cultures. Thus, a multifaceted approach, with attention to microbiological quality assurance, is needed to better guide antimicrobial use and reduce mortality and long-term impairments.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures
References
-
- Lawn JE, Blencowe H, Oza S, et al. Lancet Every Newborn Study Group Every Newborn: progress, priorities, and potential beyond survival. Lancet. 2014;384:189–205. - PubMed
-
- Goldstein B, Giroir B, Randolph A, International Consensus Conference on Pediatric Sepsis International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005;6:2–8. - PubMed
-
- Zaidi AK, Thaver D, Ali SA, et al. Pathogens associated with sepsis in newborns and young infants in developing countries. Pediatr Infect Dis J. 2009;28(1 Suppl):S10–S18. - PubMed
-
- Downie L, Armiento R, Subhi R, et al. Community-acquired neonatal and infant sepsis in developing countries: efficacy of WHO’s currently recommended antibiotics–systematic review and meta-analysis. Arch Dis Child. 2013;98:146–154. - PubMed
