

Factors associated with patient and provider delays for tuberculosis diagnosis and treatment in Asia: a systematic review and meta-analysis
- PMID: 25807385
- PMCID: PMC4373856
- DOI: 10.1371/journal.pone.0120088
Factors associated with patient and provider delays for tuberculosis diagnosis and treatment in Asia: a systematic review and meta-analysis
Abstract
Background: Delays in tuberculosis (TB) diagnosis and treatment is a major barrier to effective management of the disease. Determining the factors associated with patient and provider delay of TB diagnosis and treatment in Asia may contribute to TB prevention and control.
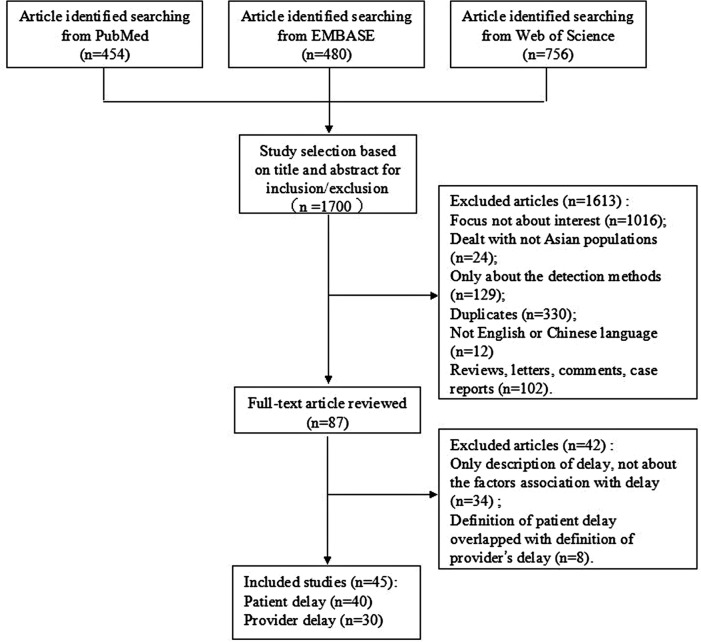
Methods: We searched the PubMed, EMBASE and Web of Science for studies that assessed factors associated with delays in care-seeking, diagnosis, or at the beginning of treatment, which were published from January 1992 to September 2014. Two reviewers independently identified studies that were related to our meta-analysis and extracted data from each study. Independent variables were categorized in separate tables for patient and provider delays.
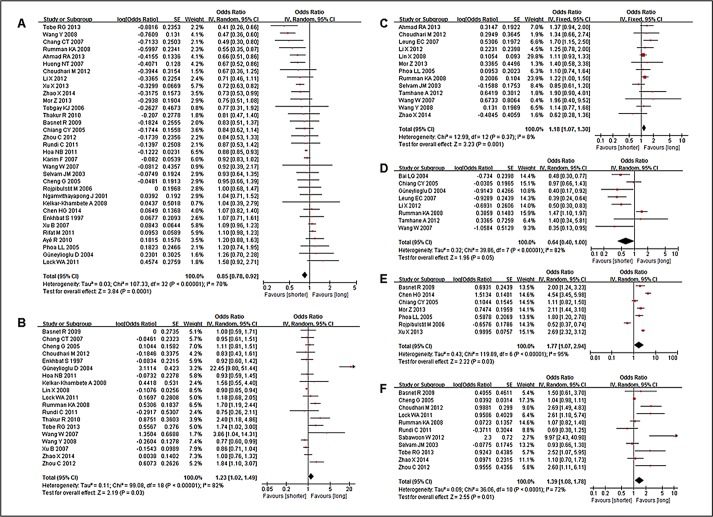
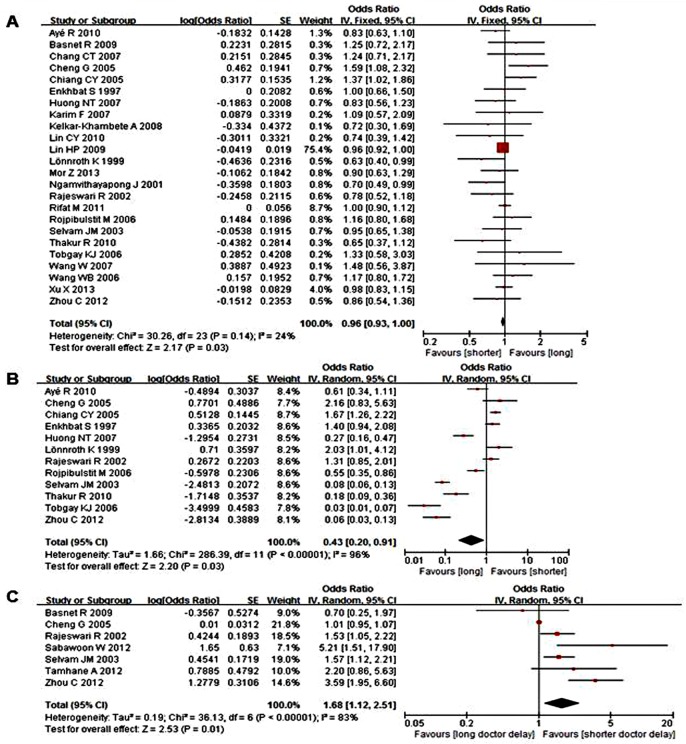
Results: Among 45 eligible studies, 40 studies assessed patient delay whereas 30 assessed provider delay. Cross-sectional surveys were used in all but two articles, which included 17 countries and regions. Socio-demographic characteristics, TB-related symptoms and medical examination, and conditions of seeking medical care in TB patients were frequently reported. Male patients and long travel time/distance to the first healthcare provider led to both shorter patient delays [odds ratio (OR) (95% confidence intervals, CI) = 0.85 (0.78, 0.92); 1.39 (1.08, 1.78)] and shorter provider delays [OR (95%CI) = 0.96 (0.93, 1.00); 1.68 (1.12, 2.51)]. Unemployment, low income, hemoptysis, and positive sputum smears were consistently associated with patient delay [ORs (95%CI) = 1.18 (1.07, 1.30), 1.23 (1.02, 1.49), 0.64 (0.40, 1.00), 1.77 (1.07, 2.94), respectively]. Additionally, consultation at a public hospital was associated with provider delay [OR (95%CI) = 0.43 (0.20, 0.91)].
Conclusions: We propose that the major opportunities to reduce delays involve enabling socio-demographic factors and medical conditions. Male, unemployed, rural residence, low income, hemoptysis, positive sputum smear, and long travel time/distance significantly correlated with patient delay. Male, long travel time/distance and consultation at a public hospital were related to provider delay.
Conflict of interest statement
Figures
References
-
- Goodchild M, Sahu S, Wares F, Dewan P, Shukla RS, Chauhan LS, et al. A cost-benefit analysis of scaling up tuberculosis control in India. Int J Tuberc Lung Dis. 2011;15(3): 358–362. - PubMed
-
- WHO. China: health, poverty and economic development. 2005. Dec [cited 17 August 2014] Geneva: World Health Organization; Available: www.who.int/macrohealth/action/CMH_China.pdf.
-
- WHO. Global Tuberculosis Report 2013. 2013. Nov [cited 17 August 2014] Geneva: World Health Organization; Available: http://apps.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf.
-
- WHO. Fact sheets on tuberculosis. 2013. [cited 17 August 2014] Geneva: World Health Organization; Available: http://www.who.int/tb/publications/factsheet_global.pdf?ua=1.
-
- Bjune G. Tuberculosis in the 21st century: an emerging pandemic? Nor Epidemiol. 2005;15(2): 133–139.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
