

A controlled resuscitation strategy is feasible and safe in hypotensive trauma patients: results of a prospective randomized pilot trial
- PMID: 25807399
- PMCID: PMC4375962
- DOI: 10.1097/TA.0000000000000600
A controlled resuscitation strategy is feasible and safe in hypotensive trauma patients: results of a prospective randomized pilot trial
Abstract
Background: Optimal resuscitation of hypotensive trauma patients has not been defined. This trial was performed to assess the feasibility and safety of controlled resuscitation (CR) versus standard resuscitation (SR) in hypotensive trauma patients.
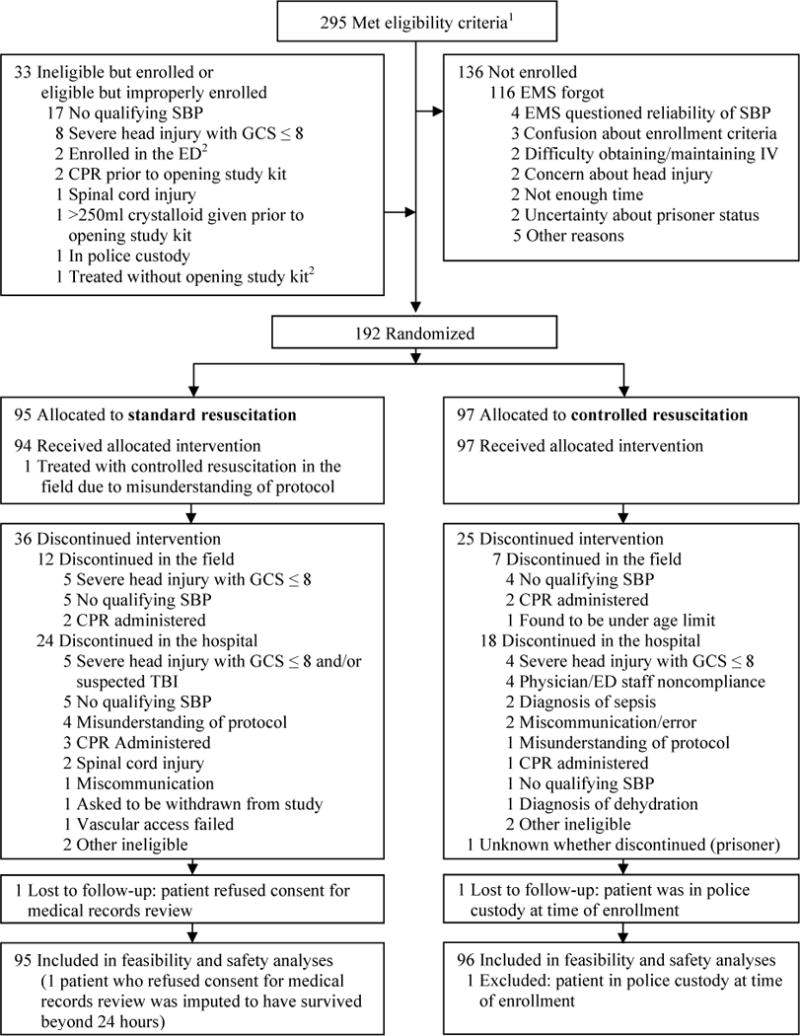
Methods: Patients were enrolled and randomized in the out-of-hospital setting. Nineteen emergency medical services (EMS) systems in the Resuscitation Outcome Consortium participated. Eligible patients had an out-of-hospital systolic blood pressure (SBP) of 90 mm Hg or lower. CR patients received 250 mL of fluid if they had no radial pulse or an SBP lower than 70 mm Hg and additional 250-mL boluses to maintain a radial pulse or an SBP of 70 mm Hg or greater. The SR group patients received 2 L initially and additional fluid as needed to maintain an SBP of 110 mm Hg or greater. The crystalloid protocol was maintained until hemorrhage control or 2 hours after hospital arrival.
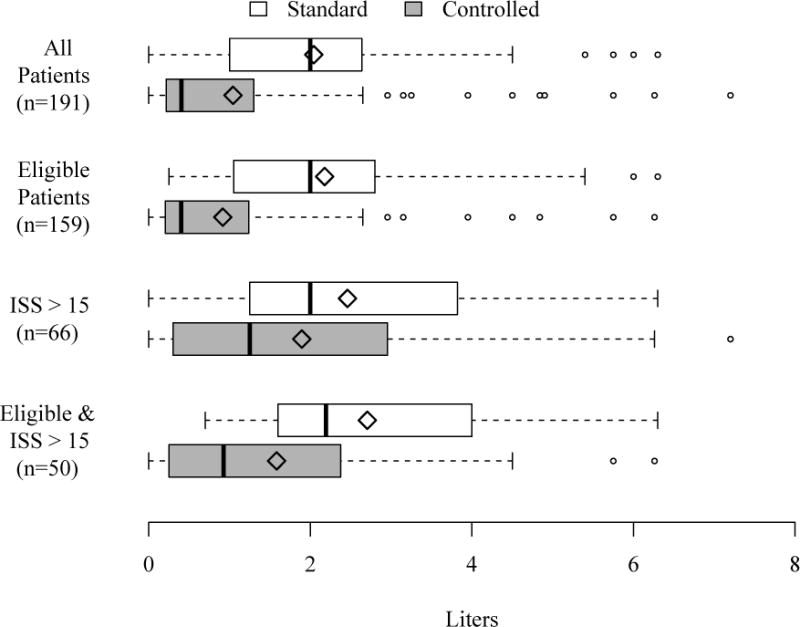
Results: A total of 192 patients were randomized (97 CR and 95 SR). The CR and SR groups were similar at baseline. The mean (SD) crystalloid volume administered during the study period was 1.0 L (1.5) in the CR group and 2.0 L (1.4) in the SR group, a difference of 1.0 L (95% confidence interval [CI], 0.6-1.4). Intensive care unit-free days, ventilator-free days, renal injury, and renal failure did not differ between the groups. At 24 hours after admission, there were 5 deaths (5%) in the CR group and 14 (15%) in the SR group (adjusted odds ratio, 0.39; 95% CI, 0.12-1.26). Among patients with blunt trauma, 24-hour mortality was 3% (CR) and 18% (SR) with an adjusted odds ratio of 0.17 (0.03-0.92). There was no difference among patients with penetrating trauma (9% vs. 9%; adjusted odds ratio, 1.93; 95% CI, 0.19-19.17).
Conclusion: CR is achievable in out-of-hospital and hospital settings and may offer an early survival advantage in blunt trauma. A large-scale, Phase III trial to examine its effects on survival and other clinical outcomes is warranted.
Level of evidence: Therapeutic study, level I.
Figures
References
-
- Bonnie R, Fulco C, Liverman C. Anonymous. Washington D.C.: National Acadamy Press; 1999. Reducing the Burden of Injury Advancing Prevention and Treatment. - PubMed
-
- Stewart RM, Myers JG, Dent DL, Ermis P, Gray GA, Villarreal R, Blow O, Woods B, McFarland M, Garavaglia J, et al. Seven hundred fifty-three consecutive deaths in a level I trauma center: The argument for injury prevention. J Trauma. 2003;54:66–70. - PubMed
-
- MacLeod JB, Cohn SM, Johnson EW, McKenney MG. Trauma deaths in the first hour: Are they all unsalvageable injuries? Am J Surg. 2007;193:195–199. - PubMed
-
- Champion HR. Combat fluid resuscitation: Introduction and overview of conferences. J Trauma. 2003;54:S7–12. - PubMed
-
- Takaori M, Safar P. Treatment of massive hemorrhage with colloid and crystalloid solutions. studies in dogs. JAMA. 1967;199:297–302. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- U01 HL077871/HL/NHLBI NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- Canadian Institutes of Health Research/Canada
- HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- 5U01 HL077863/HL/NHLBI NIH HHS/United States
- HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
