

Cerebrospinal fluid markers reveal intrathecal inflammation in progressive multiple sclerosis
- PMID: 25808056
- PMCID: PMC5568079
- DOI: 10.1002/ana.24408
Cerebrospinal fluid markers reveal intrathecal inflammation in progressive multiple sclerosis
Abstract
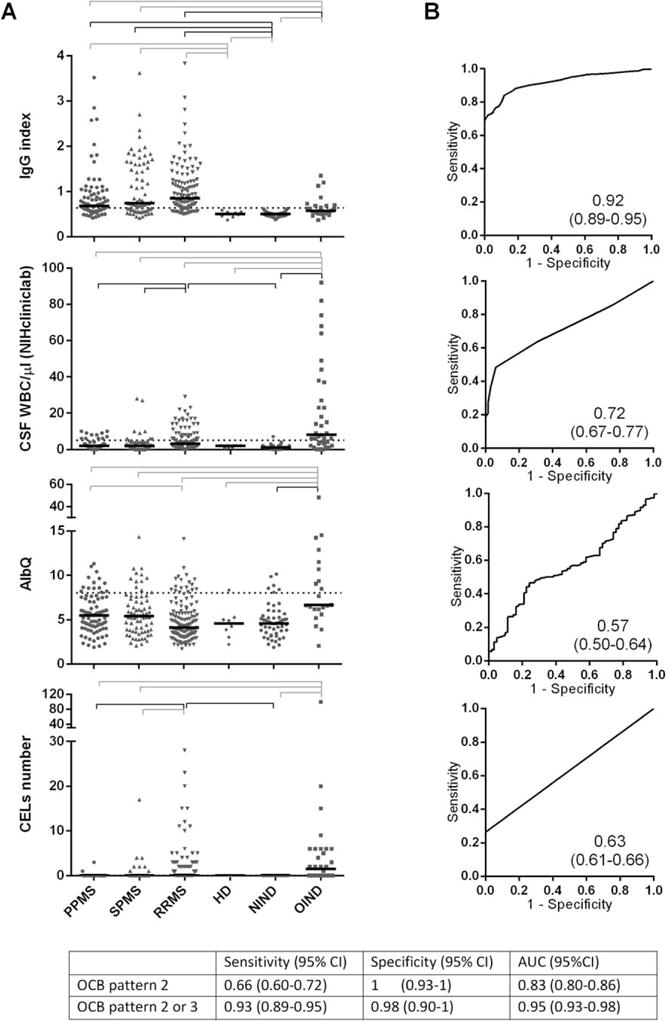
Objective: The management of complex patients with neuroimmunological diseases is hindered by an inability to reliably measure intrathecal inflammation. Currently implemented laboratory tests developed >40 years ago either are not dynamic or fail to capture low levels of central nervous system (CNS) inflammation. Therefore, we aimed to identify and validate biomarkers of CNS inflammation in 2 blinded, prospectively acquired cohorts of untreated patients with neuroimmunological diseases and embedded controls, with the ultimate goal of developing clinically useful tools.
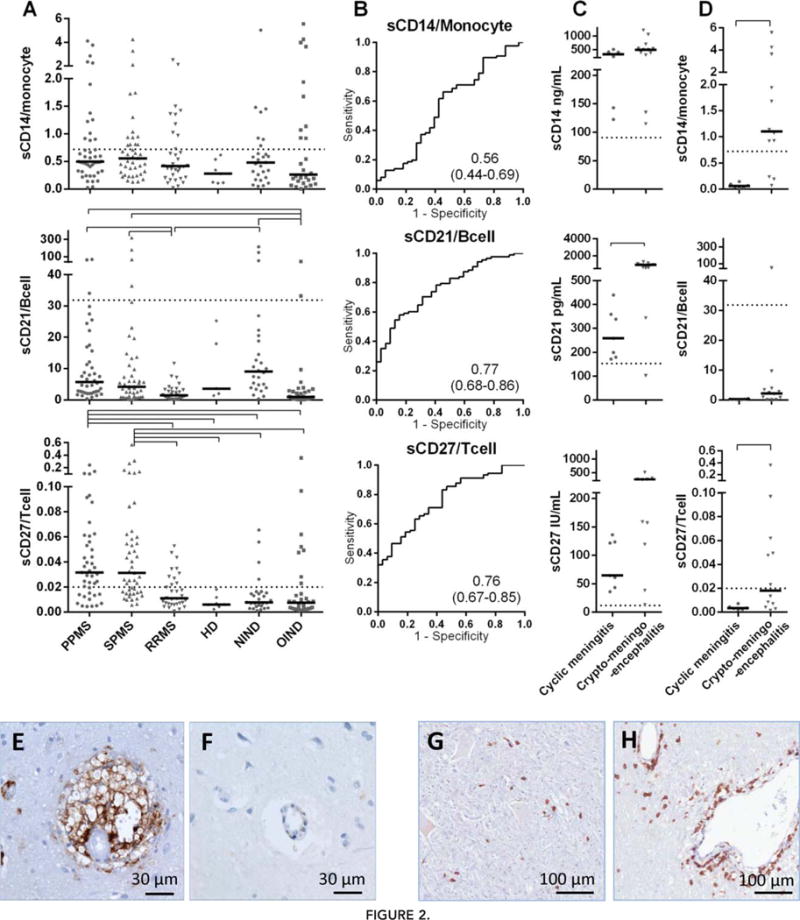
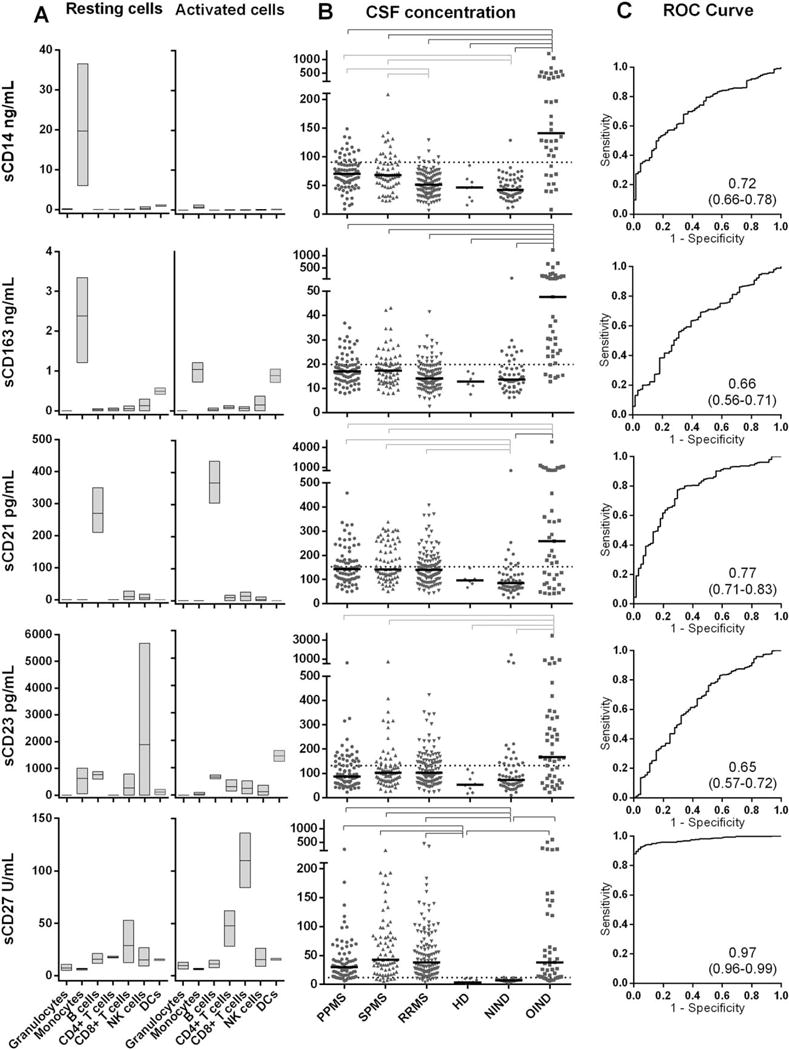
Methods: Because biomarkers with maximum utility reflect immune phenotypes, we included an assessment of cell specificity in purified primary immune cells. Biomarkers were quantified by optimized electrochemiluminescent immunoassays.
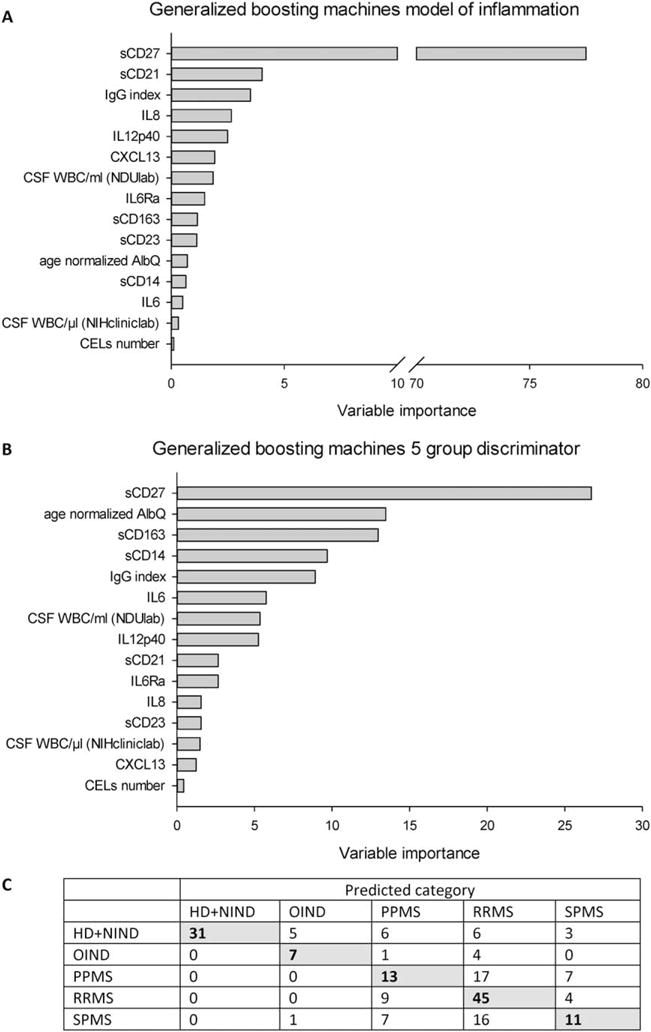
Results: Among markers with cell-specific secretion, soluble CD27 is a validated biomarker of intrathecal T-cell activation, with an area under the receiver operating characteristic curve of 0.97. Comparing the quantities of cerebrospinal fluid (CSF) immune cells and their respective cell-specific soluble biomarkers (released by CSF cells as well as their counterparts in CNS tissue) provided invaluable information about stationary CNS immune responses, previously attainable via brain biopsy only. Unexpectedly, progressive and relapsing-remitting multiple sclerosis (MS) patients have comparable numbers of activated intrathecal T and B cells, which are preferentially embedded in CNS tissue in the former group.
Interpretation: The cell-specific biomarkers of intrathecal inflammation may improve diagnosis and management of neuroimmunological diseases and provide pharmacodynamic markers for future therapeutic developments in patients with intrathecal inflammation that is not captured by imaging, such as in progressive MS.
Published 2015. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
Nothing to report.
Figures


References
-
- Sormani MP, Bruzzi P. MRI lesions as a surrogate for relapses in multiple sclerosis: a meta-analysis of randomised trials. Lancet Neurol. 2013;12:669–676. - PubMed
-
- Filippi M, Rocca MA, Barkhof F, et al. Association between pathological and MRI findings in multiple sclerosis. Lancet Neurol. 2012;11:349–360. - PubMed
-
- Stangel M, Fredrikson S, Meinl E, et al. The utility of cerebrospinal fluid analysis in patients with multiple sclerosis. Nat Rev Neurol. 2013;9:267–276. - PubMed
-
- Petzold A. Intrathecal oligoclonal IgG synthesis in multiple sclerosis. J Neuroimmunol. 2013;262:1–10. - PubMed
-
- Axelsson M, Mattsson N, Malmestrom C, et al. The influence of disease duration, clinical course, and immunosuppressive therapy on the synthesis of intrathecal oligoclonal IgG bands in multiple sclerosis. J Neuroimmunol. 2013;264:100–105. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
