

Review
doi: 10.1126/scitranslmed.aaa6853.
Advances and challenges in immunotherapy for solid organ and hematopoietic stem cell transplantation
Affiliations
- PMID: 25810312
- PMCID: PMC4425354
- DOI: 10.1126/scitranslmed.aaa6853
Item in Clipboard
Review
Advances and challenges in immunotherapy for solid organ and hematopoietic stem cell transplantation
Sci Transl Med.
.
Abstract
Although major advances have been made in solid organ and hematopoietic stem cell transplantation in the last 50 years, big challenges remain. This review outlines the current immunological limitations for hematopoietic stem cell and solid organ transplantation and discusses new immune-modulating therapies in preclinical development and in clinical trials that may allow these obstacles to be overcome.
Copyright © 2015, American Association for the Advancement of Science.
Figures
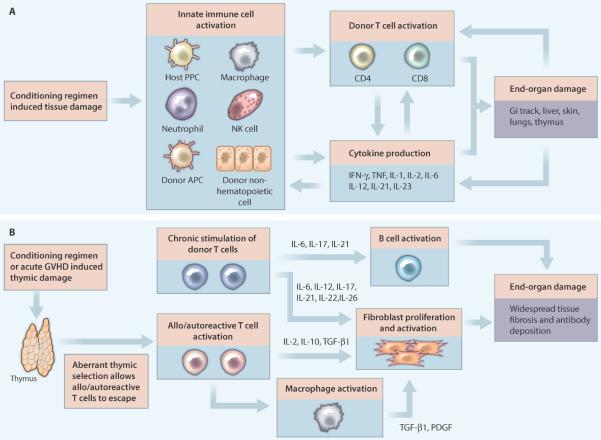
Shown are the immune processes and molecules involved in the development of (A) acute or (B) chronic GVHD after HSCT. (A) Acute GVHD begins with a conditioning regimen such as chemotherapy combined with total body irradiation that induces tissue damage. This tissue damage causes the release of danger signals, such as cytokines and chemokines, which activate recipient innate immune cells, including antigen presenting cells (APCs). Donor APCs, which are a component of the stem cell graft, are also activated by this highly inflammatory milieu. A combination of donor and recipient APCs then activate donor CD4 and CD8 T cells. Cytokine production and direct cytolysis of host cells by these T cells, as well as by host macrophages, neutrophils and natural killer (NK) cells, causes end-organ damage. The resulting tissue destruction further amplifies acute GVHD, creating a positive-feedback loop that can be difficult to stop, even with immunosuppressive drug treatment. (B) Thymic destruction, either from pre-transplant conditioning or acute GVHD, and chronic stimulation of donor T cells contribute to chronic GVHD after HSCT. Thymic damage alters the selection of T cells, which can result in the release of lymphocytes that react to host tissues. Depending upon the antigen, this reaction to host can be considered allo- or auto-reactive. Once activated, these T cells stimulate fibroblast proliferation and macrophage activation, both of which result in tissue fibrosis. Donor T cells also contribute to fibroblast activation, and play a key role in activating B cells, which produce antibodies with specificities for host tissues. All of these events contribute to the highly fibrotic syndrome of chronic GVHD.
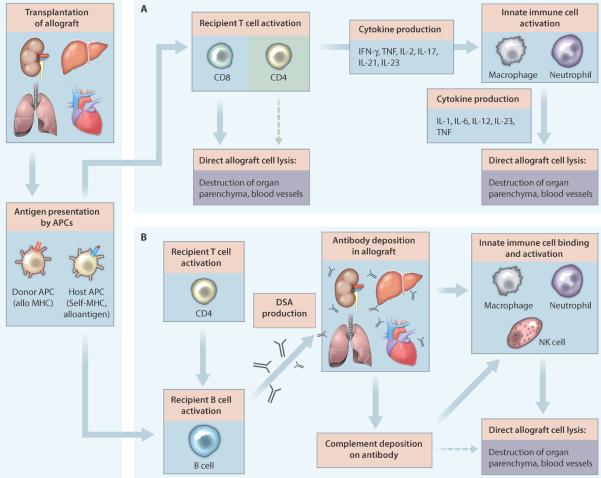
Shown are the factors involved in the development of (A) acute and (B) chronic rejection of solid organ transplants. (A) The process of acute allograft rejection begins with recipient CD4 and CD8 T cells becoming activated through interactions with donor and recipient antigen presenting cells (APCs) (respectively termed direct and indirect allorecognition). After activation, CD8 T cells, and to a lesser extent CD4 T cells, directly destroy both graft blood vessels and parenchyma. Recipient CD4 T cells primarily contribute to acute rejection by producing a variety of cytokines that activate macrophages and neutrophils. These innate cells then attack and lyse graft cells. The combination of lymphocyte and innate cell directed graft destruction results in allograft dysfunction and acute rejection. (B) In chronic allograft rejection, CD4 T cells help to induce antibody class switching, affinity maturation, and ultimately the production of donor-specific antibodies (DSA) by recipient B cells. Binding of donor-specific antibodies to graft cells enhances neutrophil, macrophage and NK cell-mediated destruction of the graft (via Fc receptor binding) and results in complement deposition. Subsequent activation of the complement cascade results in direct lysis of graft cells via the complement membrane attack complex and further augments innate cell recognition and destruction of the graft. Although this process evolves over months to years, it results in chronic allograft dysfunction and eventual complete rejection. PDGF, platelet derived growth factor.
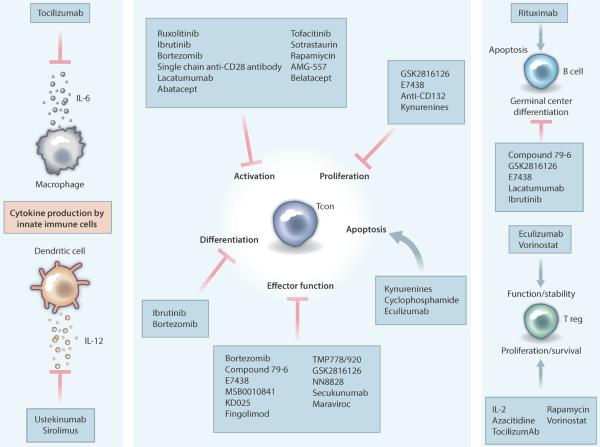
Shown are known mechanisms by which new agents alter critical aspects of the pathogenesis of GVHD and solid organ transplant rejection. The majority of these therapies focus on inhibiting various functions of conventional T cells, which are the primary drivers of many aspects of GVHD and allograft rejection. Abatacept, belatacept: CTLA-4Ig fusion protein inhibitors of CD80/86; azacitidine, DNA hypomethylating agent; sotrastaurin, pan-PKC inhibitor with preferential selectivity for PKC-theta; anti-CD132, anti-IL-2 common gamma chain (CD132) mAb; AMG557, anti- ICOS/B7RP1 mAb; bortezomib, proteasome inhibitor; compound 79-6, Bcl-6 inhibitor; cyclophosphamide, DNA alkylating agent; E7438, EZH2 methyltransferase inhibitor; eculizumab, complement inhibitor; fingolimod, sphingosine-1-phosphate receptor inhibitor; GSK2816126, an EZH2 methyltransferase inhibitor; ibrutinib, BTK/ITK inhibitor; KD025, ROCK2 inhibitor; kynurenines, products of L-tryptophan catabolism; lucatumumab, anti-CD40 mAb; maraviroc, CCR5 antagonist; MSB0010841, anti-IL-17A/F nanobody; NN8828, anti-IL-21 mAb; rapamycin, mTOR inhibitor; rituximab, anti-CD20 mAb; ruxolitinib, JAK1/2 inhibitor; single-chain anti-CD28 antibody, anti-CD28 mAb; TMP778, RAR-related orphan receptor gamma-t (RORgt) antagonist; TMP920, RORgt antagonist; tocilizumab, anti-IL-6R mAb; tofacitinib, JAK3 inhibitor; ustekinumab, anti-IL-12/23 mAb; vorinostat/suberanilohydroxamic acid, HDAC inhibitor. HDAC, histone deacetylase; Tcon, conventional T cell; Treg, regulatory T cell; mAb, monoclonal antibody.
References
-
- Pasquini M, Wang Z. “Current use and outcome of hematopoietic stem cell transplantation: CIBMTR Summary Slides, 2014,”. 2014 Available at http://www.cibmtr.org.
-
- Welniak LA, Blazar BR, Murphy WJ. Immunobiology of Allogeneic Hematopoietic Stem Cell Transplantation. Annual Review of Immunology. 2007;25:139–170. - PubMed
Publication types
MeSH terms
Grants and funding
- UM1 AI109565/AI/NIAID NIH HHS/United States
- P01 CA065493/CA/NCI NIH HHS/United States
- R01 HL118979/HL/NHLBI NIH HHS/United States
- R01 AI034495/AI/NIAID NIH HHS/United States
- R01 AI037691/AI/NIAID NIH HHS/United States
- R01 HL056067/HL/NHLBI NIH HHS/United States
- R01 AI112613/AI/NIAID NIH HHS/United States
- R01 CA072669/CA/NCI NIH HHS/United States
- P01 CA142106/CA/NCI NIH HHS/United States
- P01 AI056299/AI/NIAID NIH HHS/United States
- T32 AI007313/AI/NIAID NIH HHS/United States
- F30 HL121873/HL/NHLBI NIH HHS/United States
- R37 AI034495/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
