

How I treat priapism
- PMID: 25810489
- PMCID: PMC4458797
- DOI: 10.1182/blood-2014-09-551887
How I treat priapism
Abstract
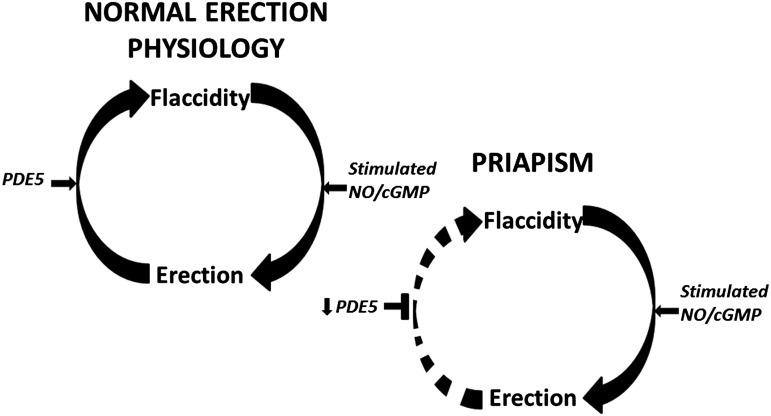
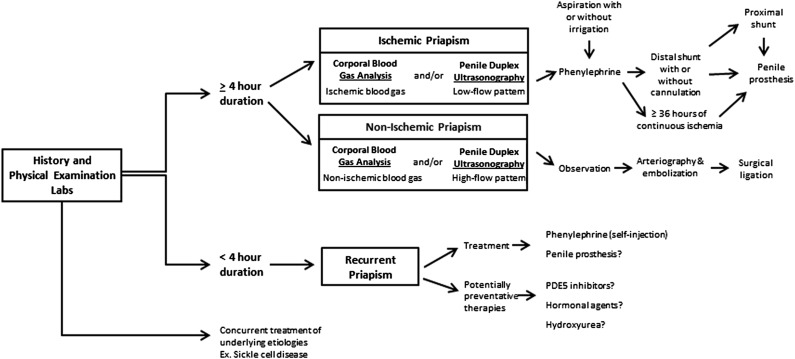
Priapism is a disorder of persistent penile erection unrelated to sexual interest or desire. This pathologic condition, specifically the ischemic variant, is often associated with devastating complications, notably erectile dysfunction. Because priapism demonstrates high prevalence in patients with hematologic disorders, most commonly sickle cell disease (SCD), there is significant concern for its sequelae in this affected population. Thus, timely diagnosis and management are critical for the prevention or at least reduction of cavernosal tissue ischemia and potential damage consequent to each episode. Current guidelines and management strategies focus primarily on reactive treatments. However, an increasing understanding of the molecular pathophysiology of SCD-associated priapism has led to the identification of new potential therapeutic targets. Future agents are being developed and explored for use in the prevention of priapism.
© 2015 by The American Society of Hematology.
Figures
References
-
- Berger R, Billups K, Brock G, et al. AFUD Thought Leader Panel on Evaluation and Treatment of Priapism. Report of the American Foundation for Urologic Disease (AFUD) Thought Leader Panel for evaluation and treatment of priapism. Int J Impot Res. 2001;13(suppl 5):S39–S43. - PubMed
-
- Montague DK, Jarow J, Broderick GA, et al. Members of the Erectile Dysfunction Guideline Update Panel; Americal Urological Association. American Urological Association guideline on the management of priapism. J Urol. 2003;170(4 pt 1):1318–1324. - PubMed
-
- Morrison BF, Burnett AL. Priapism in hematological and coagulative disorders: an update. Nat Rev Urol. 2011;8(4):223–230. - PubMed
-
- Burnett AL, Bivalacqua TJ. Priapism: current principles and practice. Urol Clin North Am. 2007;34(4):631–642, viii. - PubMed
-
- Eland IA, van der Lei J, Stricker BH, Sturkenboom MJ. Incidence of priapism in the general population. Urology. 2001;57(5):970–972. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
