Efficacy versus health risks: An in vitro evaluation of power-driven scalers
- PMID: 25810588
- PMCID: PMC4365149
- DOI: 10.4103/0972-124X.145796
Efficacy versus health risks: An in vitro evaluation of power-driven scalers
Abstract
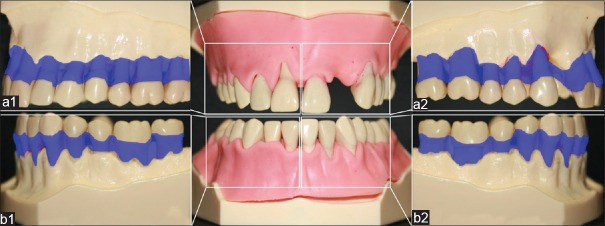
Background: Power-driven instrumentation of root surfaces during supportive periodontal therapy is an alternative to hand instrumentation. The purpose of this pilot in vitro study was to investigate the efficacy of sub- and supragingival plaque removal with a sonic (AIR: Synea, W and H, Bürmoos, Austria) and two ultrasonic devices (TIG: Tigon+, W and H, Bürmoos, Austria; VEC: Vector, Dürr, Bietigheim-Bissingen, Germany) as well as the health-risk for dental professionals during treatment.
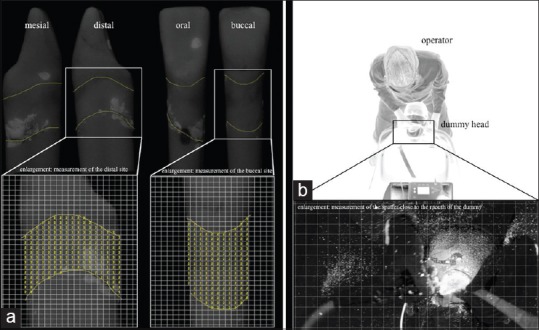
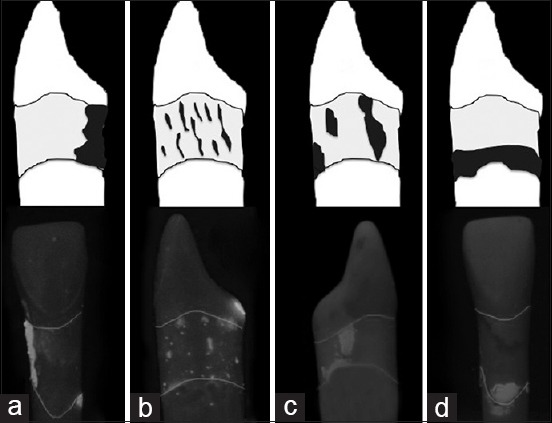
Materials and methods: The power-driven devices were utilized to remove plaque from model teeth in dummy heads. The percentage of residual artificial plaque after 2 min of supra- or subgingival instrumentation was calculated by means of image-processing techniques at four sites (n = 576) of each tooth. The Health-Risk-Index (HRI: spatter/residual plaque quotient) with the different power-driven devices was assessed during treatment.
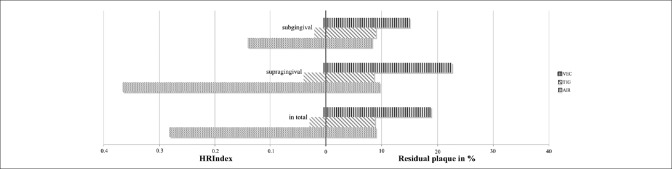
Results: The smallest amounts of residual plaque were found for the sonic device AIR (8.89% ± 10.92%) and the ultrasonic scaler TIG (8.72% ± 12.02%) (P = 0.707). Significantly more plaque was remained after the use of the ultrasonic scaler VEC (18.76% ± 18.07%) (P < 0.001). Irrespectively of the scaler, efficacy was similar sub- (10.7% ± 11.6%) and supragingivally (13.5% ± 17.2%) (P = 0.901). AIR/TIG demonstrated equal residual amounts of plaque sub- (P = 0.831) as well as supragingivally (P = 0.510). However, AIR/VEC and TIG/VEC were significantly in favor of AIR and TIG (P < 0.001). In contrast, the lowest HRI was found after using VEC (0.0043) and differed considerably for AIR (0.2812) and TIG (0.0287).
Conclusion: Sonic devices are as effective as ultrasonic devices in the removal of biofilm but bear a higher risk to the dental professional's health concerning the formation of spatter.
Keywords: Aerosol; dental prophylaxis; plaque; scaling.
Conflict of interest statement
Figures


Similar articles
-
Removal of simulated biofilm: an evaluation of the effect on root surfaces roughness after scaling.Clin Oral Investig. 2017 May;21(4):1021-1028. doi: 10.1007/s00784-016-1861-9. Epub 2016 May 27. Clin Oral Investig. 2017. PMID: 27233902
-
Spatter contamination in dental practices--how can it be prevented?Rev Med Chir Soc Med Nat Iasi. 2014 Oct-Dec;118(4):1122-34. Rev Med Chir Soc Med Nat Iasi. 2014. PMID: 25581979 Clinical Trial.
-
Subgingival instrumentation to remove simulated plaque in vitro: influence of operators' experience and type of instrument.Clin Oral Investig. 2015 Jun;19(5):987-95. doi: 10.1007/s00784-014-1319-x. Epub 2014 Sep 19. Clin Oral Investig. 2015. PMID: 25231069 Clinical Trial.
-
Root instrumentation. Power-driven versus manual scalers, which one?Dent Clin North Am. 1998 Apr;42(2):229-44. Dent Clin North Am. 1998. PMID: 9597335 Review.
-
Position paper: sonic and ultrasonic scalers in periodontics. Research, Science and Therapy Committee of the American Academy of Periodontology.J Periodontol. 2000 Nov;71(11):1792-801. doi: 10.1902/jop.2000.71.11.1792. J Periodontol. 2000. PMID: 11128930 Review.
Cited by
-
Demystifying the mist: Sources of microbial bioload in dental aerosols.J Periodontol. 2020 Sep;91(9):1113-1122. doi: 10.1002/JPER.20-0395. Epub 2020 Jul 27. J Periodontol. 2020. PMID: 32662070 Free PMC article. Review.
-
Influence of Adjunctive Photodynamic Therapy on Interleukin-6, Interleukin-8, and Interleukin-10 Gingival Crevicular Fluid Levels in Chronic Periodontitis - A Randomized Controlled Trial.Contemp Clin Dent. 2021 Jul-Sep;12(3):235-240. doi: 10.4103/ccd.ccd_510_20. Epub 2021 Sep 21. Contemp Clin Dent. 2021. PMID: 34759679 Free PMC article.
-
Removal of simulated biofilm: a preclinical ergonomic comparison of instruments and operators.Clin Oral Investig. 2016 Jul;20(6):1193-201. doi: 10.1007/s00784-015-1605-2. Epub 2015 Sep 29. Clin Oral Investig. 2016. PMID: 26416709
-
Removal of simulated biofilm: an evaluation of the effect on root surfaces roughness after scaling.Clin Oral Investig. 2017 May;21(4):1021-1028. doi: 10.1007/s00784-016-1861-9. Epub 2016 May 27. Clin Oral Investig. 2017. PMID: 27233902
-
Dental Aerosol as a Hazard Risk for Dental Workers.Materials (Basel). 2020 Nov 12;13(22):5109. doi: 10.3390/ma13225109. Materials (Basel). 2020. PMID: 33198307 Free PMC article.
References
-
- Kocher T, Rühling A, Momsen H, Plagmann HC. Effectiveness of subgingival instrumentation with power-driven instruments in the hands of experienced and inexperienced operators. A study on manikins. J Clin Periodontol. 1997;24:498–504. - PubMed
-
- Tunkel J, Heinecke A, Flemmig TF. A systematic review of efficacy of machine-driven and manual subgingival debridement in the treatment of chronic periodontitis. J Clin Periodontol. 2002;29(Suppl 3):72–81. - PubMed
-
- Legnani P, Checchi L, Pelliccioni GA, D’Achille C. Atmospheric contamination during dental procedures. Quintessence Int. 1994;25:435–9. - PubMed
-
- Bentley CD, Burkhart NW, Crawford JJ. Evaluating spatter and aerosol contamination during dental procedures. J Am Dent Assoc. 1994;125:579–84. - PubMed