

Facial nerve paralysis: A case report of rare complication in uncontrolled diabetic patient with mucormycosis
- PMID: 25810669
- PMCID: PMC4367044
- DOI: 10.4103/0976-9668.149195
Facial nerve paralysis: A case report of rare complication in uncontrolled diabetic patient with mucormycosis
Abstract
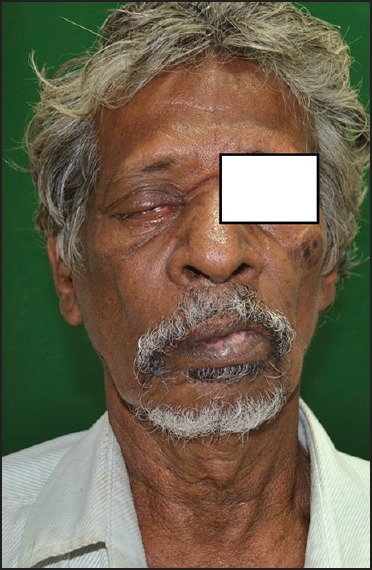
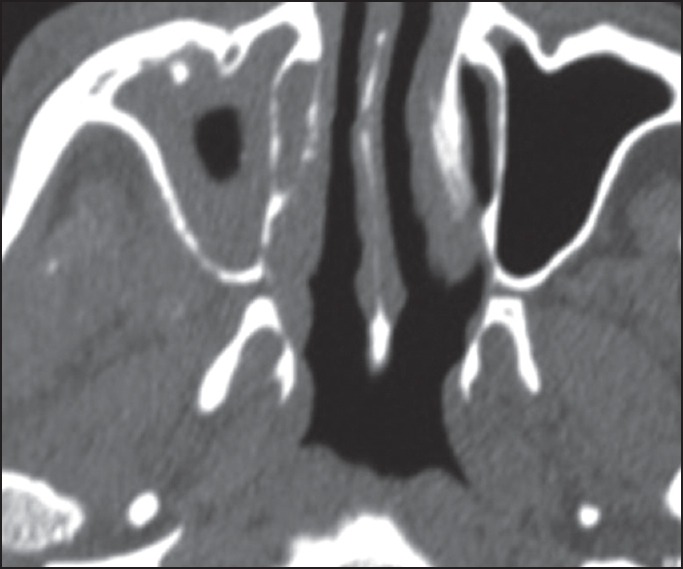
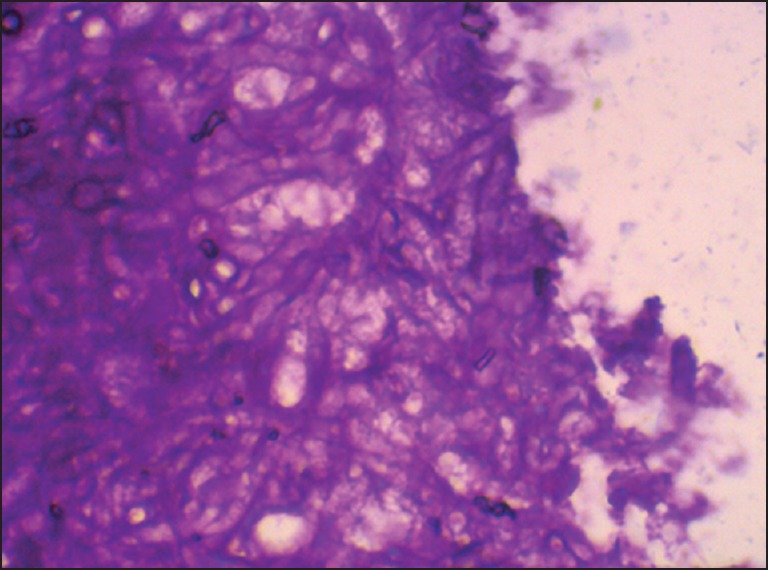
Mucormycosis is a rare opportunistic aggressive and fatal infection caused by mucor fungus. Seven types of mucormycosis are identified based on the extension and involvement of the lesion, of which the rhino orbital mucormycosis is most common in the head and neck region. Although it is widely spread in nature, clinical cases are rare and observed only in immunocompromised patients and patients with uncontrolled diabetes mellitus. Early symptoms include fever, nasal ulceration or necrosis, periorbital edema or facial swelling, paresthesia and reduced vision. Involvement of cranial nerves although not common, facial nerve palsy is a rare finding. The infection may spread through cribriform plate to the brain resulting in extensive cerebellar infarctions. Timely diagnosis and early recognition of the signs and symptoms, correction of underlying medical disorders, and aggressive medical and surgical intervention are necessary for successful therapeutic outcome.
Keywords: Diabetes mellitus; facial nerve palsy; mucormycosis.
Conflict of interest statement
Figures

References
-
- Santos Gorjón P, Blanco Pérez P, Batuecas Caletrío A, Muñoz Herrera AM, Sánchez González F, de la Fuente Cañibano R. Rhino-orbito-cerebral mucormycosis, a retrospective study of 7 cases. Acta Otorrinolaringol Esp. 2010;61:48–53. - PubMed
-
- Koc Z, Koc F, Yerdelen D, Ozdogu H. Rhino-orbital-cerebral mucormycosis with different cerebral involvements: Infarct, hemorrhage, and ophthalmoplegia. Int J Neurosci. 2007;117:1677–90. - PubMed
-
- Cohen SG, Greenberg MS. Rhinomaxillary mucormycosis in a kidney transplant patient. Oral Surg Oral Med Oral Pathol. 1980;50:33–8. - PubMed
-
- Davis RL, Robertson DM. 2nd ed. Baltimore: Williams & Wilkins; 1991. Textbook of Neuropathology; pp. 761–3.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources