

Mild hyperthermia influence on Herceptin(®) properties
- PMID: 25810700
- PMCID: PMC4362605
- DOI: 10.2478/raon-2014-0045
Mild hyperthermia influence on Herceptin(®) properties
Abstract
Background: Mild hyperthermia (mHT) increases the tumor perfusion and vascular permeability, and reduces the interstitial fluid pressure, resulting in better intra-tumoral bioavailability of low molecular weight drugs. This approach is potentially also attractive for delivery of therapeutic macromolecules, such as antibodies. Here, we investigated the effects of mHT on the stability, immunological and pharmacological properties of Herceptin(®), a clinically approved antibody, targeting the human epidermal growth factor receptor 2 (HER-2) overexpressed in breast cancer.
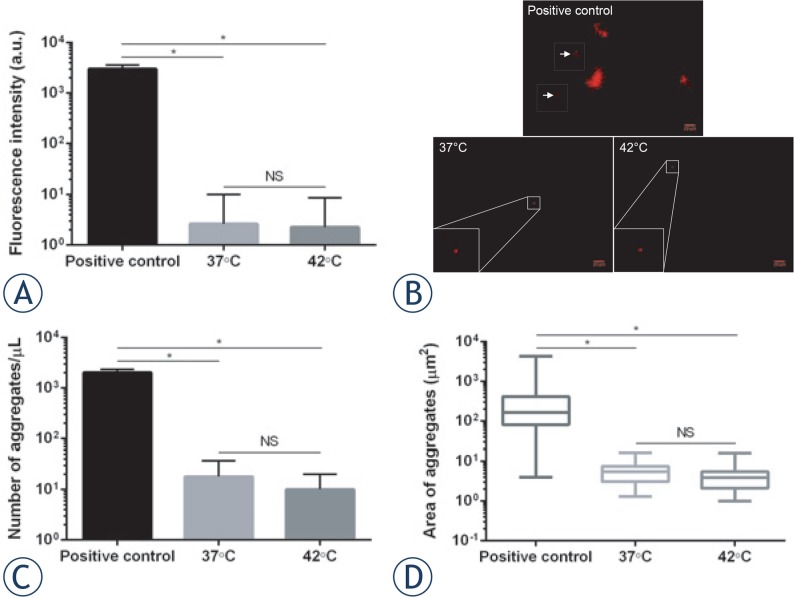
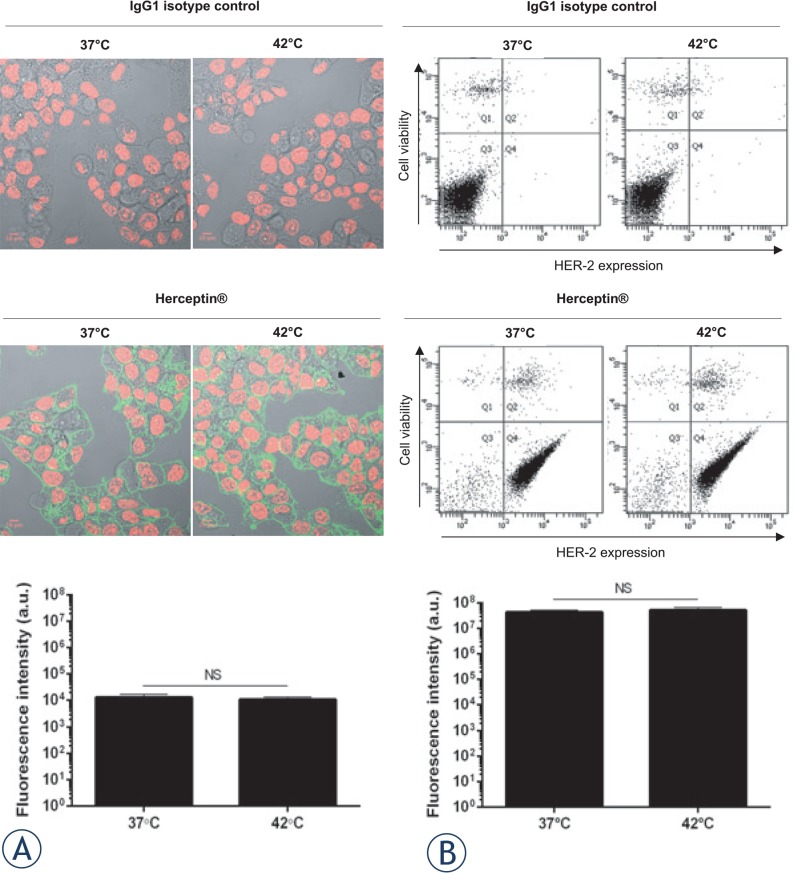
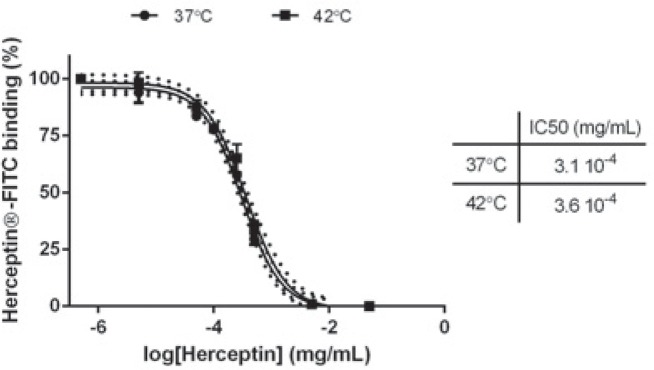
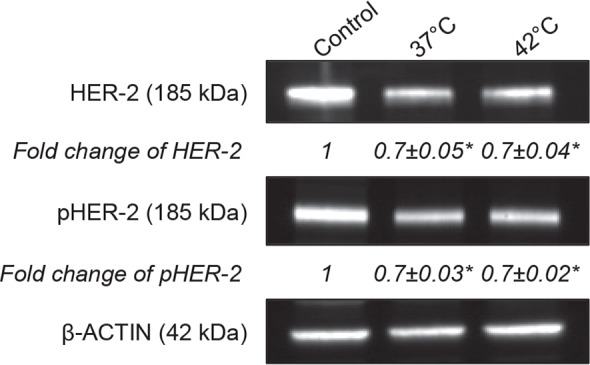
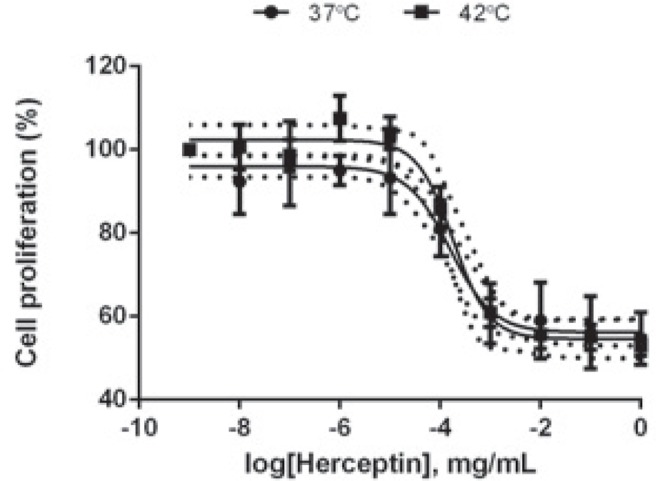
Results: Herceptin(®) was heated to 37°C (control) and 42°C (mHT) for 1 hour. Formation of Herceptin(®) aggregates was measured using Nile Red assay. mHT did not result in additional Herceptin(®) aggregates compared to 37°C, showing the Herceptin(®) stability is unchanged. Immunological and pharmacological properties of Herceptin(®) were evaluated following mHT using HER-2 positive breast cancer cells (BT-474). Exposure of Herceptin(®) to mHT preserved recognition and binding affinity of Herceptin(®) to HER-2. Western-blot and cell proliferation assays on BT-474 cells showed that mHT left the inhibitory activities of Herceptin(®) unchanged.
Conclusions: The stability, and the immunological and pharmacological properties of Herceptin(®) are not negatively affected by mHT. Further in-vivo studies are required to evaluate the influence of mHT on intra-tumoral bioavailability and therapeutic effectiveness of Herceptin(®).
Keywords: Herceptin®; anticancer antibody; breast cancer; mild hyperthermia.
Figures
References
-
- Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, Rosso S, Coebergh JW, Comber H, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49:1374–403. - PubMed
-
- Arteaga CL, Sliwkowski MX, Osborne CK, Perez EA, Puglisi F, Gianni L. Treatment of HER2-positive breast cancer: current status and future perspectives. Nat Rev Clin Oncol. 2012;9:16–32. - PubMed
-
- Eroles P, Bosch A, Perez-Fidalgo JA, Lluch A. Molecular biology in breast cancer: intrinsic subtypes and signaling pathways. Cancer Treat Rev. 2012;38:698–707. - PubMed
-
- Hudis CA. Trastuzumab-mechanism of action and use in clinical practice. N Engl J Med. 2007;357:39–51. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous