

Prognosis for Spontaneous Resolution of OSA in Children
- PMID: 25811889
- PMCID: PMC4631037
- DOI: 10.1378/chest.14-2873
Prognosis for Spontaneous Resolution of OSA in Children
Abstract
Background: Adenotonsillectomy (AT) is commonly performed for childhood OSA syndrome (OSAS), but little is known about prognosis without treatment.
Methods: The Childhood Adenotonsillectomy Trial (CHAT) randomized 50% of eligible children with OSAS to a control arm (watchful waiting), with 7-month follow-up symptom inventories, physical examinations, and polysomnography. Polysomnographic and symptomatic resolution were defined respectively by an apnea/hypopnea index (AHI) <2 and obstructive apnea index (OAI) <1 and by an OSAS symptom score (Pediatric Sleep Questionnaire [PSQ]) < 0.33 with ≥ 25% improvement from baseline.
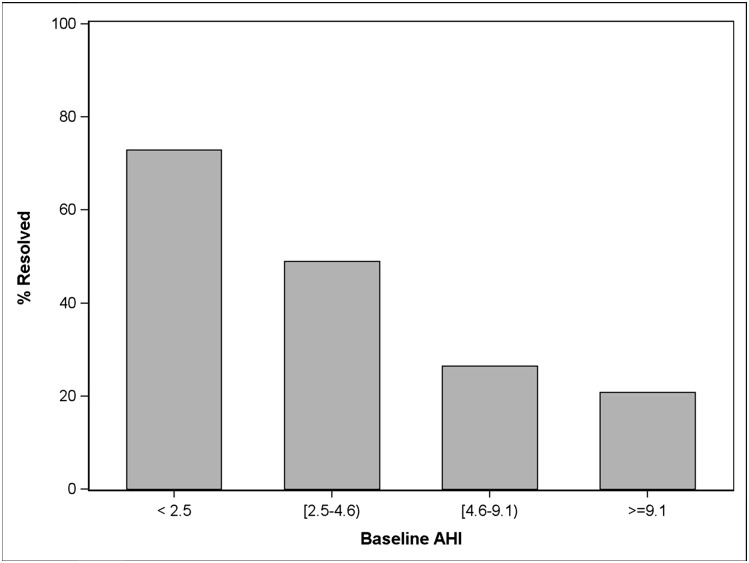
Results: After 194 children aged 5 to 9 years underwent 7 months of watchful waiting, 82 (42%) no longer met polysomnographic criteria for OSAS. Baseline predictors of resolution included lower AHI, better oxygen saturation, smaller waist circumference or percentile, higher-positioned soft palate, smaller neck circumference, and non-black race (each P < .05). Among these, the independent predictors were lower AHI and waist circumference percentile < 90%. Among 167 children with baseline PSQ scores ≥ 0.33, only 25 (15%) experienced symptomatic resolution. Baseline predictors were low PSQ and PSQ snoring subscale scores; absence of habitual snoring, loud snoring, observed apneas, or a household smoker; higher quality of life; fewer attention-deficit/hyperactivity disorder symptoms; and female sex. Only lower PSQ and snoring scores were independent predictors.
Conclusions: Many candidates for AT no longer have OSAS on polysomnography after 7 months of watchful waiting, whereas meaningful improvement in symptoms is not common. In practice, a baseline low AHI and normal waist circumference, or low PSQ and snoring score, may help identify an opportunity to avoid AT.
Trial registry: ClinicalTrials.gov; No.: NCT00560859; URL: www.clinicaltrials.gov.
Figures
Comment in
-
Childhood OSA Syndrome: Patience for Your Patients Is a Virtue.Chest. 2015 Nov;148(5):1129-1130. doi: 10.1378/chest.15-1041. Chest. 2015. PMID: 26527437 No abstract available.
References
-
- Bhattacharyya N, Lin HW. Changes and consistencies in the epidemiology of pediatric adenotonsillar surgery, 1996-2006. Otolaryngol Head Neck Surg. 2010;143(5):680-684. - PubMed
-
- Mitchell RB, Kelly J. Quality of life after adenotonsillectomy for SDB in children. Otolaryngol Head Neck Surg. 2005;133(4):569-572. - PubMed
-
- Mitchell RB, Kelly J. Behavioral changes in children with mild sleep-disordered breathing or obstructive sleep apnea after adenotonsillectomy. Laryngoscope. 2007;117(9):1685-1688. - PubMed
-
- Tran KD, Nguyen CD, Weedon J, Goldstein NA. Child behavior and quality of life in pediatric obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 2005;131(1):52-57. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
