

Transfusion and coagulation management in major obstetric hemorrhage
- PMID: 25812005
- PMCID: PMC4567035
- DOI: 10.1097/ACO.0000000000000180
Transfusion and coagulation management in major obstetric hemorrhage
Abstract
Purpose of review: Major obstetric hemorrhage is a leading cause of maternal morbidity and mortality. We will review transfusion strategies and the value of monitoring the maternal coagulation profile during severe obstetric hemorrhage.
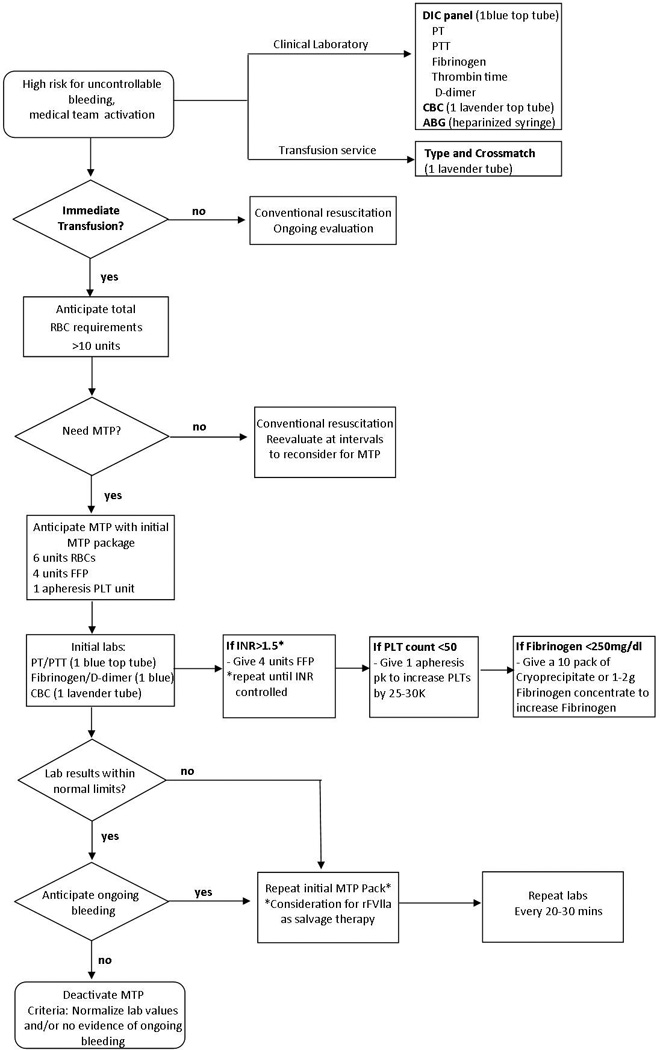
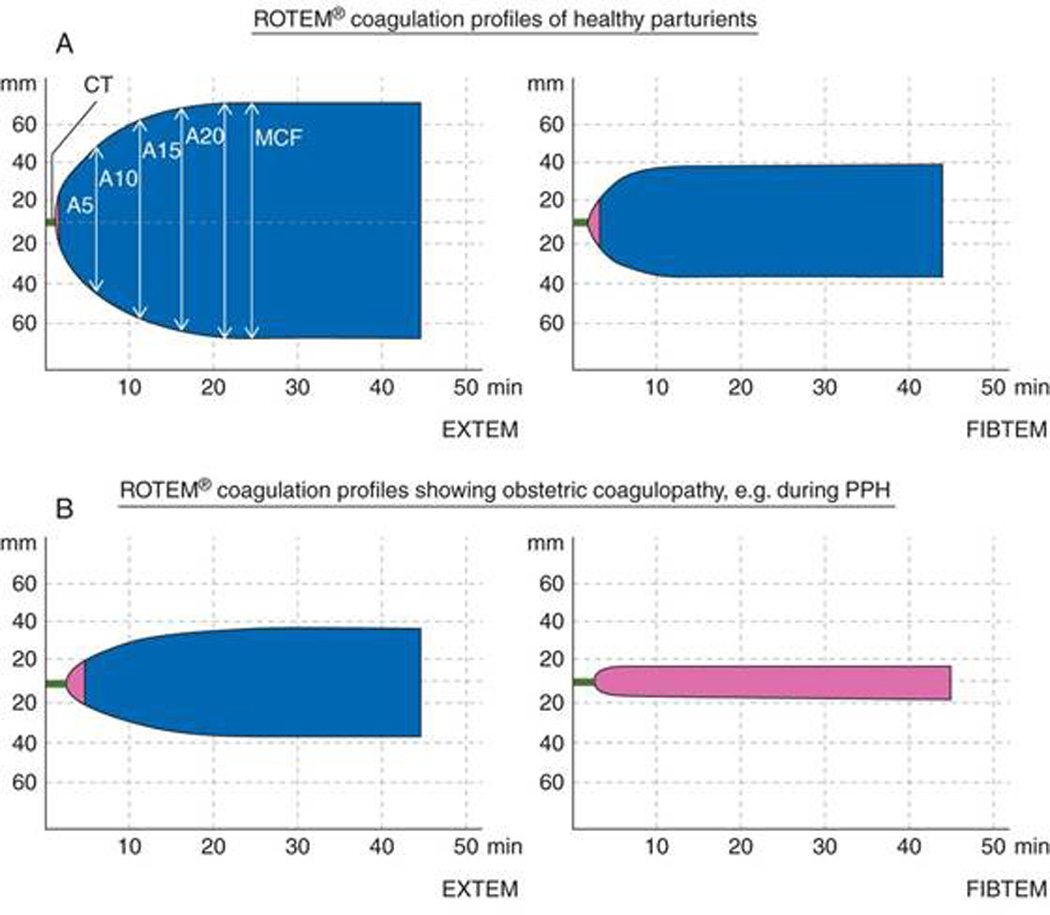
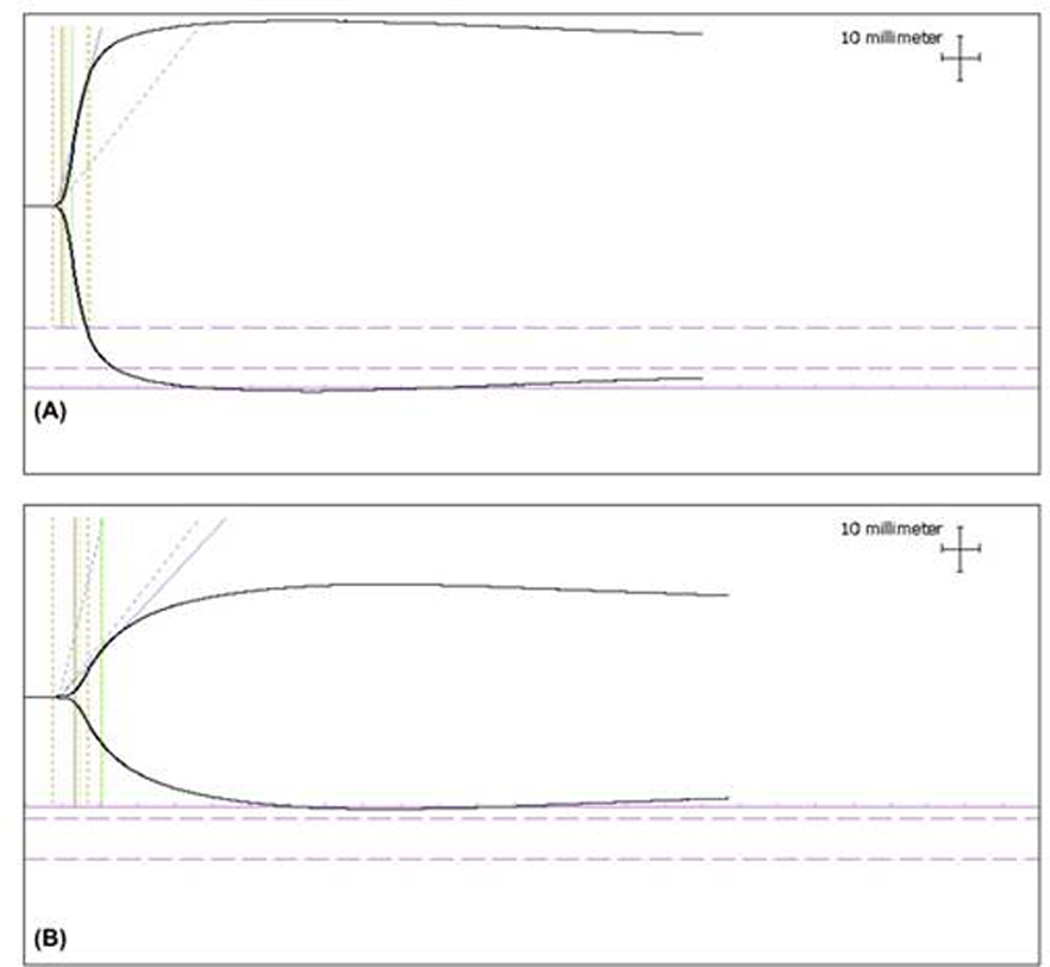
Recent findings: Epidemiologic studies indicate that rates of severe postpartum hemorrhage (PPH) in well resourced countries are increasing. Despite these increases, rates of transfusion in obstetrics are low (0.9-2.3%), and investigators have questioned whether a predelivery 'type and screen' is cost-effective for all obstetric patients. Instead, blood ordering protocols specific to obstetric patients can reduce unnecessary antibody testing. When severe PPH occurs, a massive transfusion protocol has attracted interest as a key therapeutic resource by ensuring sustained availability of blood products to the labor and delivery unit. During early postpartum bleeding, recent studies have shown that hypofibrinogenemia is an important predictor for the later development of severe PPH. Point-of-care technologies, such as thromboelastography and rotational thromboelastometry, can identify decreased fibrin clot quality during PPH, which correlate with low fibrinogen levels.
Summary: A massive transfusion protocol provides a key resource in the management of severe PPH. However, future studies are needed to assess whether formula-driven vs. goal-directed transfusion therapy improves maternal outcomes in women with severe PPH.
Figures
References
-
- Khan KS, Wojdyla D, Say L, et al. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367:1066–1074. - PubMed
-
- Cantwell R, Clutton-Brock T, Cooper G, et al. Saving Mothers' Lives: Reviewing maternal deaths to make motherhood safer: 2006–2008. The Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG. 2011;118(Suppl 1):1–203. - PubMed
-
-
Creanga AA, Berg C, Syverson C, et al. Pregnancy-related mortality in the United States, 2006–2010. Obstet Gynecol. 2015;2015:5–12. This report provides the most recent maternal mortality data in the United States between 2006–2010. In this report, 11.4% of maternal deaths were due to obstetric-related hemorrhage, with ruptured ectopic, other or unspecificied, atony or other uterine bleeding, and abnormal placentation being the most common etiologies
-
-
- Bateman BT, Berman MF, Riley LE, Leffert LR. The epidemiology of postpartum hemorrhage in a large, nationwide sample of deliveries. Anesth Analg. 2010;110:1368–1373. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
