

Effects of Statin versus the Combination of Ezetimibe plus Statin on Serum Lipid Absorption Markers in Patients with Acute Coronary Syndrome
- PMID: 25815213
- PMCID: PMC4359845
- DOI: 10.1155/2015/109158
Effects of Statin versus the Combination of Ezetimibe plus Statin on Serum Lipid Absorption Markers in Patients with Acute Coronary Syndrome
Abstract
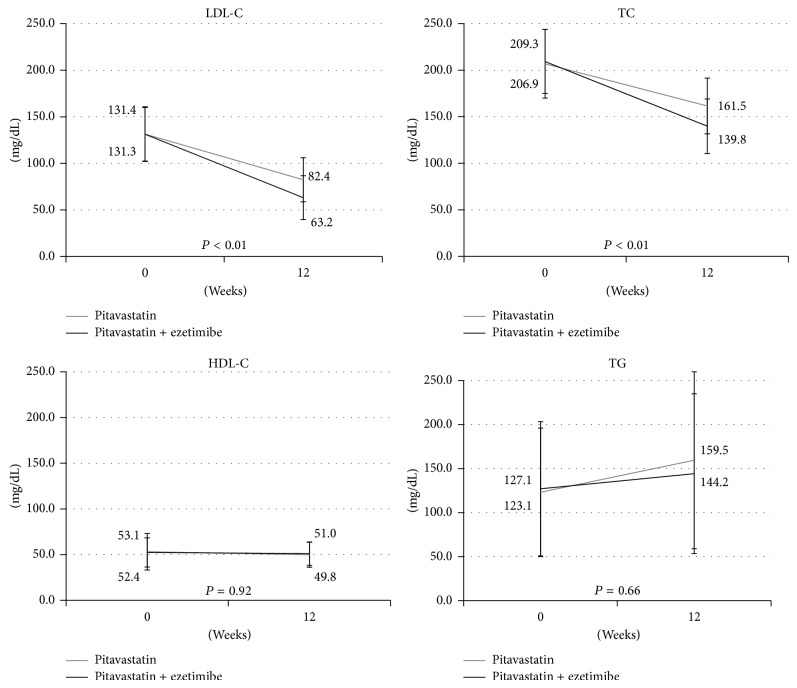
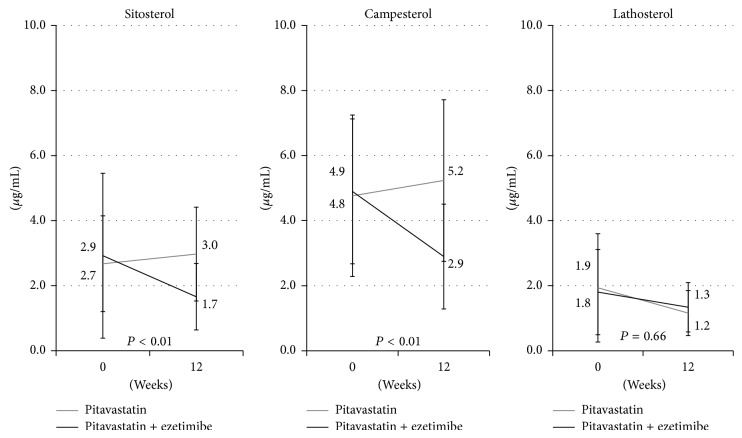
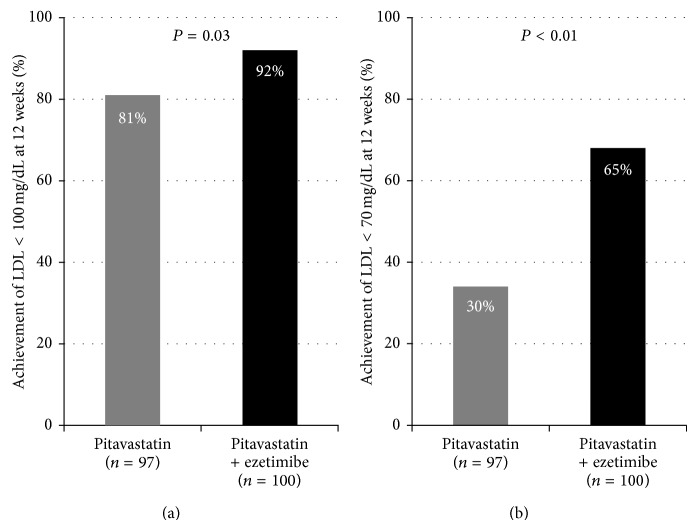
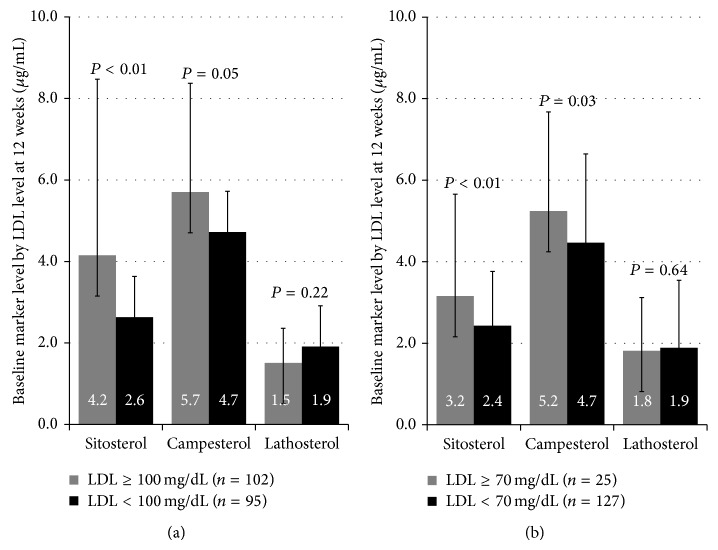
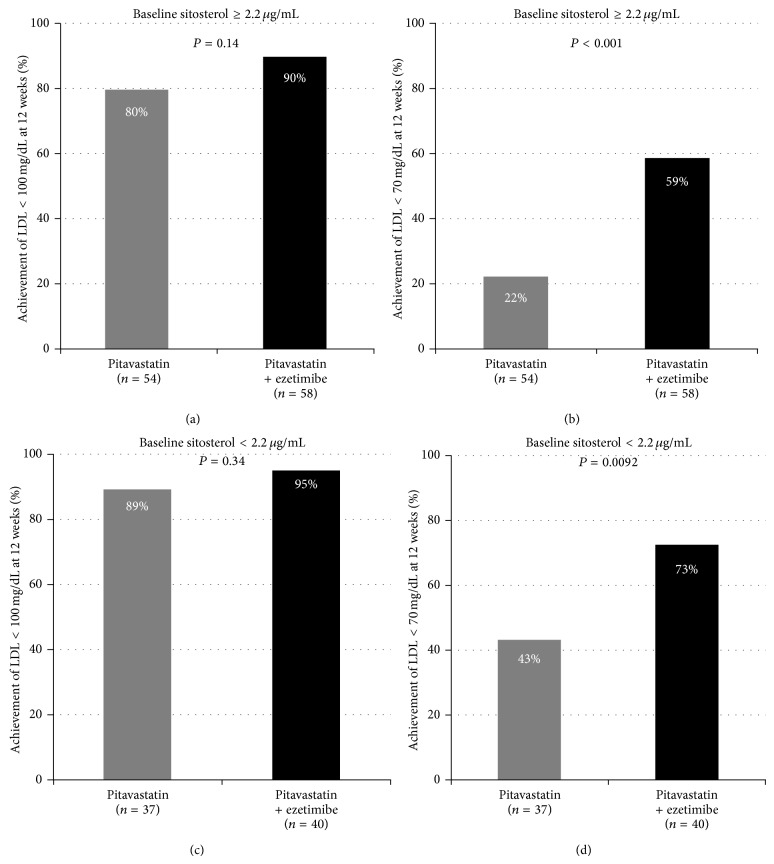
Background. The use of statins is essential for aggressive lipid-lowering treatment in acute coronary syndrome (ACS) patients with dyslipidemia. Recently, elevation of sitosterol, a lipid absorption marker, was reported to be associated with premature atherosclerosis. The purpose of the present study was to examine the impact of ezetimibe, a selective intestinal cholesterol transporter inhibitor, in ACS patients. Methods. A total of 197 ACS patients were randomized to pitavastatin + ezetimibe (n = 100) or pitavastatin (n = 97). Low-density lipoprotein cholesterol (LDL-C) and sitosterol levels were evaluated on admission and after 12 weeks. Results. After 12 weeks, the pitavastatin + ezetimibe group showed a significantly greater decrease of sitosterol (baseline versus after 12 weeks; 2.9 ± 2.5 versus 1.7 ± 1.0 ng/mL, P < 0.001) than the pitavastatin group (2.7 ± 1.5 versus 3.0 ± 1.4 ng/mL). The baseline sitosterol level was significantly higher in patients with achieved LDL-C levels ≥ 70 mg/dL than in patients with levels < 70 mg/dL (3.2 ± 2.5 versus 2.4 ± 1.3 ng/mL, P = 0.006). Conclusions. Ezetimibe plus statin therapy in ACS patients with dyslipidemia decreased LDL-C and sitosterol levels more than statin therapy solo. Sitosterol Elevation was a predictor of poor response to aggressive lipid-lowering treatment in ACS patients.
Figures
References
-
- de Lemos J. A., Blazing M. A., Wiviott S. D., et al. Early intensive vs a delayed conservative simvastatin strategy in patients with acute coronary syndromes: phase Z of the A to Z trial. The Journal of the American Medical Association. 2004;292(11):1307–1316. doi: 10.1001/jama.292.11.1307. - DOI - PubMed
-
- Matthan N. R., Resteghini N., Robertson M., et al. Cholesterol absorption and synthesis markers in individuals with and without a CHD event during pravastatin therapy: insights from the PROSPER trial. The Journal of Lipid Research. 2010;51(1):202–209. doi: 10.1194/jlr.m900032-jlr200. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
