

Early virological and immunological events in asymptomatic Epstein-Barr virus infection in African children
- PMID: 25816224
- PMCID: PMC4376400
- DOI: 10.1371/journal.ppat.1004746
Early virological and immunological events in asymptomatic Epstein-Barr virus infection in African children
Abstract
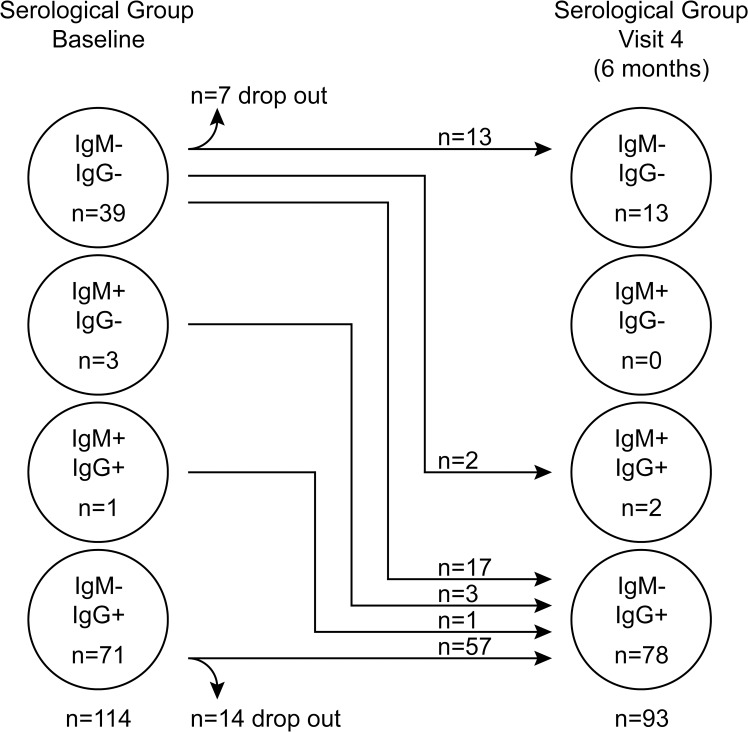
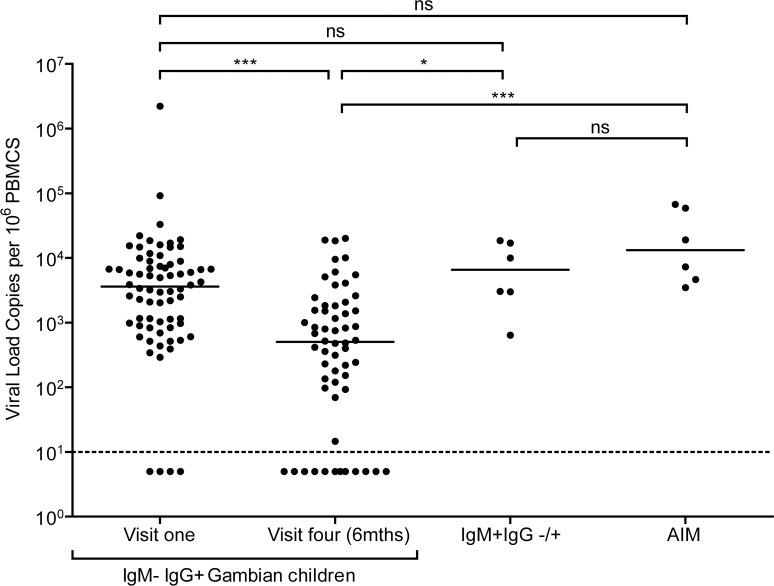
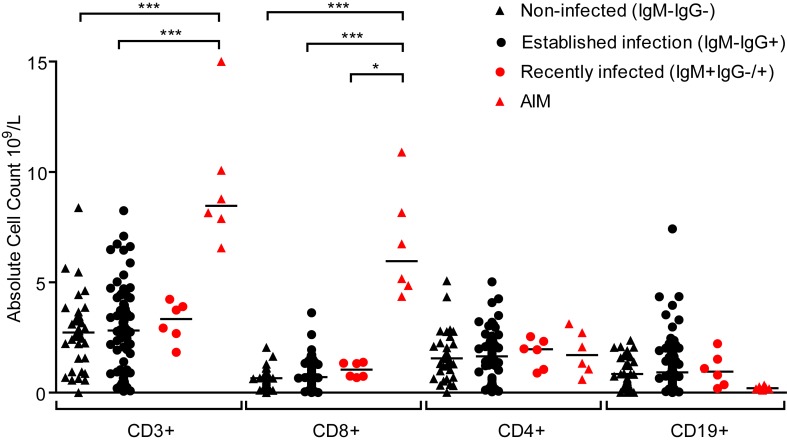
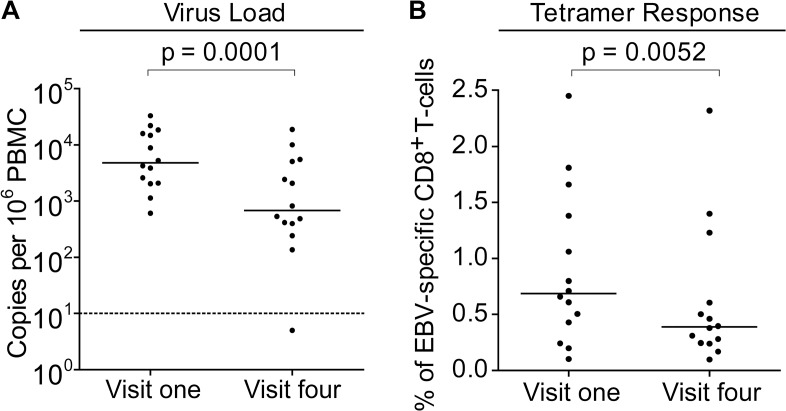
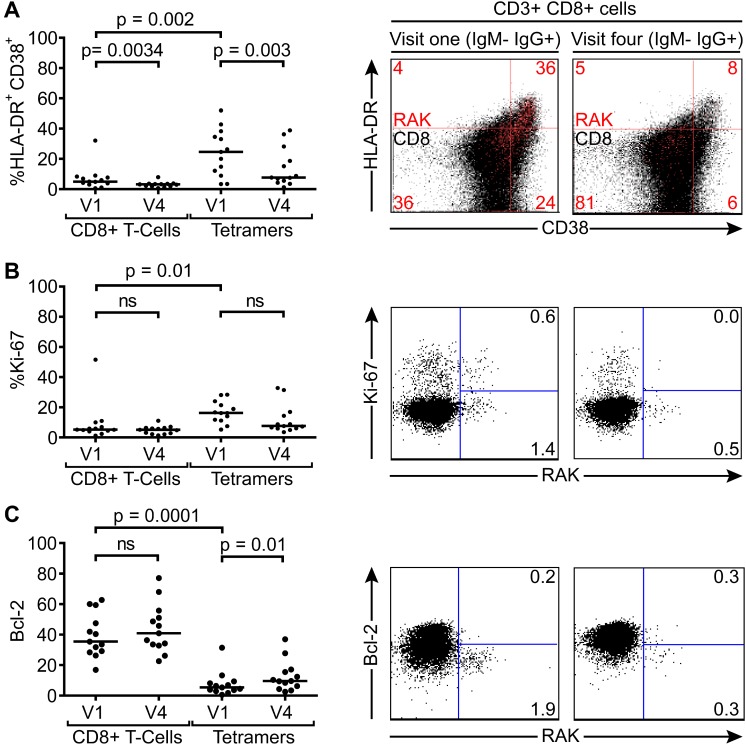
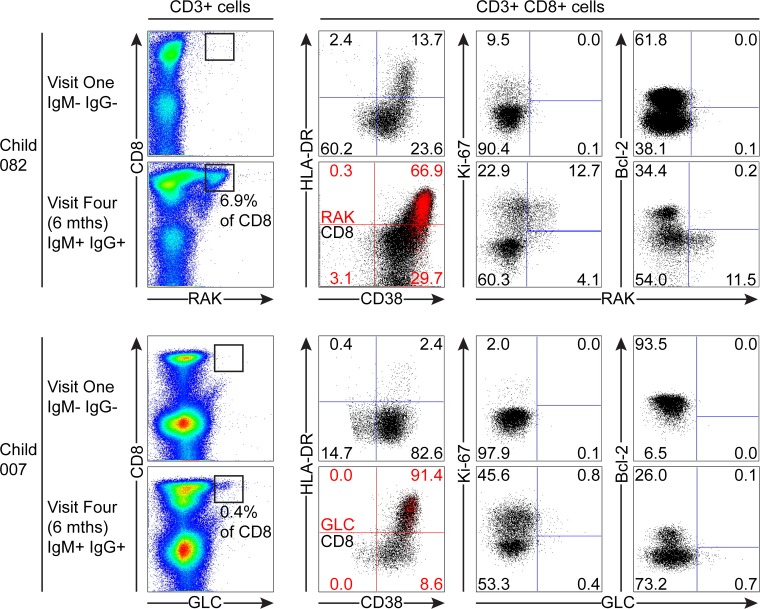
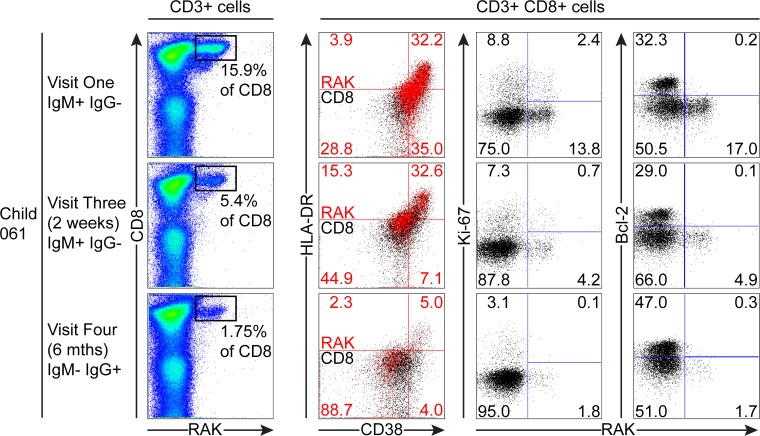
Epstein-Barr virus (EBV) infection often occurs in early childhood and is asymptomatic. However, if delayed until adolescence, primary infection may manifest as acute infectious mononucleosis (AIM), a febrile illness characterised by global CD8+ T-cell lymphocytosis, much of it reflecting a huge expansion of activated EBV-specific CD8+ T-cells. While the events of AIM have been intensely studied, little is known about how these relate to asymptomatic primary infection. Here Gambian children (14-18 months old, an age at which many acquire the virus) were followed for the ensuing six months, monitoring circulating EBV loads, antibody status against virus capsid antigen (VCA) and both total and virus-specific CD8+ T-cell numbers. Many children were IgG anti-VCA-positive and, though no longer IgM-positive, still retained high virus loads comparable to AIM patients and had detectable EBV-specific T-cells, some still expressing activation markers. Virus loads and the frequency/activation status of specific T-cells decreased over time, consistent with resolution of a relatively recent primary infection. Six children with similarly high EBV loads were IgM anti-VCA-positive, indicating very recent infection. In three of these donors with HLA types allowing MHC-tetramer analysis, highly activated EBV-specific T-cells were detectable in the blood with one individual epitope response reaching 15% of all CD8+ T-cells. That response was culled and the cells lost activation markers over time, just as seen in AIM. However, unlike AIM, these events occurred without marked expansion of total CD8+ numbers. Thus asymptomatic EBV infection in children elicits a virus-specific CD8+ T-cell response that can control the infection without over-expansion; conversely, in AIM it appears the CD8 over-expansion, rather than virus load per se, is the cause of disease symptoms.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Biggar RJ, Henle G, Bocker J, Lennette ET, Fleisher G, et al. (1978) Primary Epstein-Barr virus infections in African infants. II. Clinical and serological observations during seroconversion. Int J Cancer 22: 244–250. - PubMed
-
- Hislop AD, Taylor GS, Sauce D, Rickinson AB (2007) Cellular responses to viral infection in humans: lessons from Epstein-Barr virus. Annu Rev Immunol 25: 587–617. - PubMed
-
- Crawford DH, Macsween KF, Higgins CD, Thomas R, McAulay K, et al. (2006) A cohort study among university students: identification of risk factors for Epstein-Barr virus seroconversion and infectious mononucleosis. Clin Infect Dis 43: 276–282. - PubMed
-
- Sumaya CV, Henle W, Henle G, Smith MH, LeBlanc D (1975) Seroepidemiologic study of Epstein-Barr virus infections in a rural community. J Infect Dis 131: 403–408. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
