

Early hemostatic responses to trauma identified with hierarchical clustering analysis
- PMID: 25816845
- PMCID: PMC4452397
- DOI: 10.1111/jth.12919
Early hemostatic responses to trauma identified with hierarchical clustering analysis
Abstract
Background: Trauma-induced coagulopathy is a complex multifactorial hemostatic response that is poorly understood.
Objectives: To identify distinct hemostatic responses to trauma and identify key components of the hemostatic system that vary between responses.
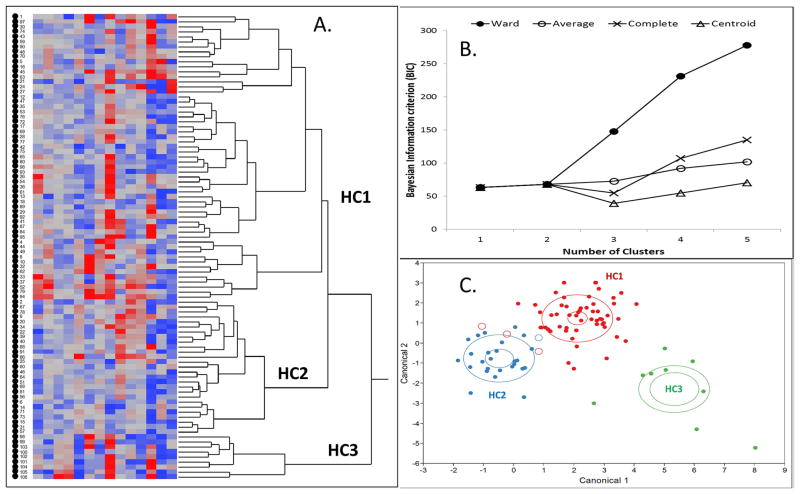
Patients/methods: A cross-sectional observational study of adult trauma patients at an urban level I trauma center emergency department was performed. Hierarchical clustering analysis was used to identify distinct clusters of similar subjects according to vital signs, injury/shock severity, and comprehensive assessment of coagulation, clot formation, platelet function, and thrombin generation.
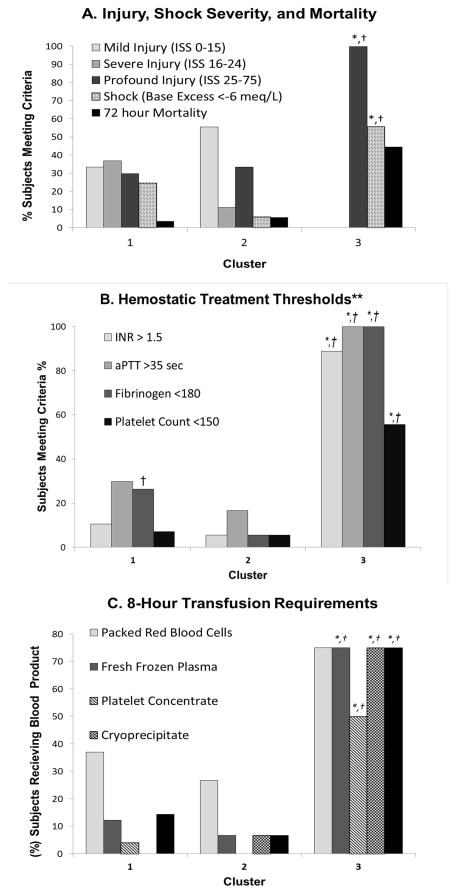
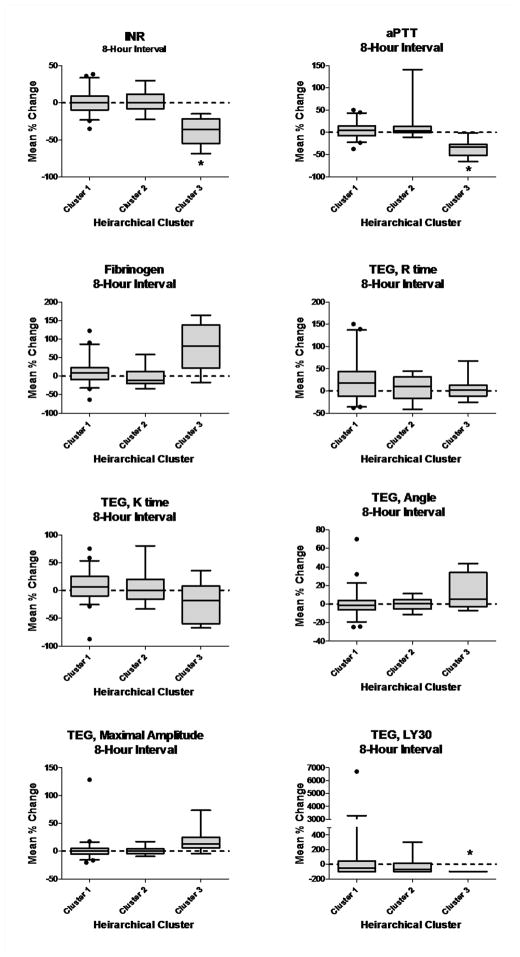
Results: Among 84 total trauma patients included in the model, three distinct trauma clusters were identified. Cluster 1 (N = 57) showed platelet activation, preserved peak thrombin generation, plasma coagulation dysfunction, a moderately decreased fibrinogen concentration and normal clot formation relative to healthy controls. Cluster 2 (N = 18) showed platelet activation, preserved peak thrombin generation, and a preserved fibrinogen concentration with normal clot formation. Cluster 3 (N = 9) was the most severely injured and shocked, and showed a strong inflammatory and bleeding phenotype. Platelet dysfunction, thrombin inhibition, plasma coagulation dysfunction and a decreased fibrinogen concentration were present in this cluster. Fibrinolytic activation was present in all clusters, but was particularly increased in cluster 3. Trauma clusters were most noticeably different in their relative fibrinogen concentration, peak thrombin generation, and platelet-induced clot contraction.
Conclusions: Hierarchical clustering analysis identified three distinct hemostatic responses to trauma. Further insights into the underlying hemostatic mechanisms responsible for these responses are needed.
Keywords: coagulation; fibrinogen; hemostasis; platelets; thrombin; trauma.
© 2015 International Society on Thrombosis and Haemostasis.
Conflict of interest statement
N. J. White reports grants from iTrauma Care Inc., Life Science Discovery Fund, Coulter Foundation and KITECH; and personal fees from Vidacare and CSL Behring, outside the submitted work. In addition, N. J. White has a patent from University of Washington licensed to Stasys Medical Corp for a platelet diagnostic device, and a patent from University of Washington for a hemostatic biopolymer.
Figures
References
-
- Jenkins DH, Rappold JF, Badloe JF, Berséus O, Blackbourne L, Brohi KH, Butler FK, Cap AP, Cohen MJ, Davenport R, DePasquale M, Doughty H, Glassberg E, Hervig T, Hooper TJ, Kozar R, Maegele M, Moore EE, Murdock A, Ness PM. Trauma hemostasis and oxygenation research position paper on remote damage control resuscitation: definitions, current practice, and knowledge gaps. Shock. 2014;41:3–12. - PMC - PubMed
-
- Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma Acute Care Surg. 2003;54:1127–1130. - PubMed
-
- Cardenas JC1, Matijevic N, Baer LA, Holcomb JB, Cotton BA, Wade CE. Elevated tissue plasminogen activator and reduced plasminogen activator inhibitor promote hyperfibrinolysis in trauma patients. Shock. 2014;41:514–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
