

Pivotal preclinical trial of the spheroid reservoir bioartificial liver
- PMID: 25817557
- PMCID: PMC4508211
- DOI: 10.1016/j.jhep.2015.03.021
Pivotal preclinical trial of the spheroid reservoir bioartificial liver
Abstract
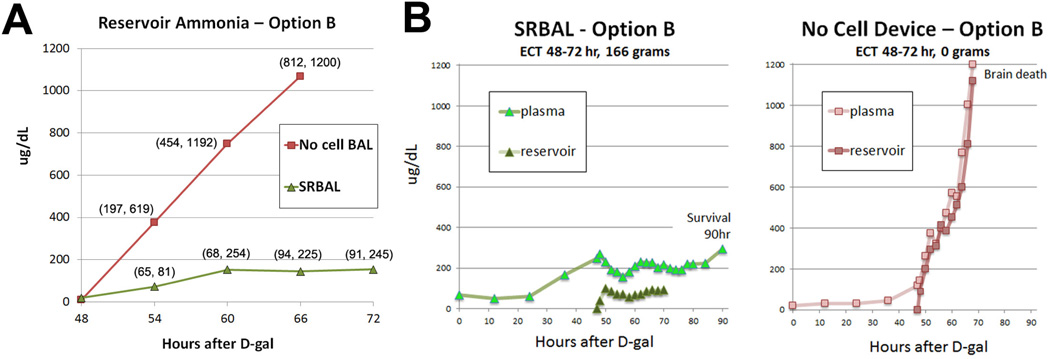
Background & aims: The neuroprotective effect of the spheroid reservoir bioartificial liver (SRBAL) was evaluated in a porcine model of drug-overdose acute liver failure (ALF).
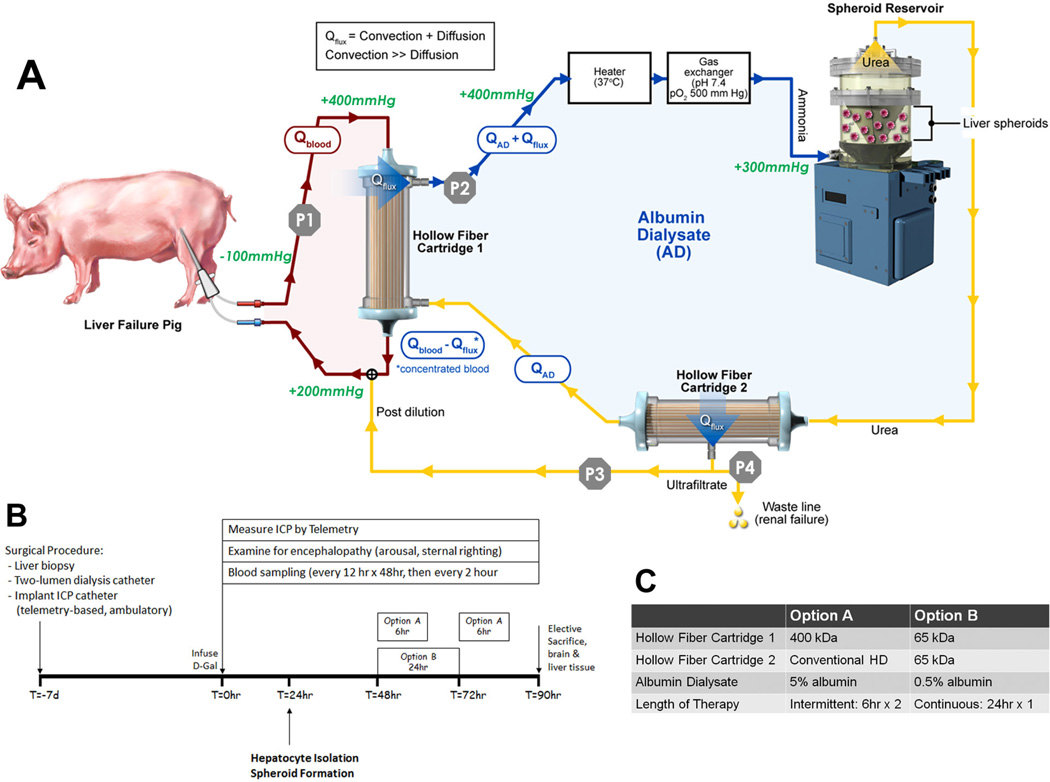
Methods: Healthy pigs were randomized into three groups (standard therapy (ST) alone, ST+No-cell device, ST+SRBAL device) before placement of an implantable intracranial pressure (ICP) monitor and a tunneled central venous catheter. One week later, pigs received bolus infusion of the hepatotoxin D-galactosamine and were followed for up to 90h.
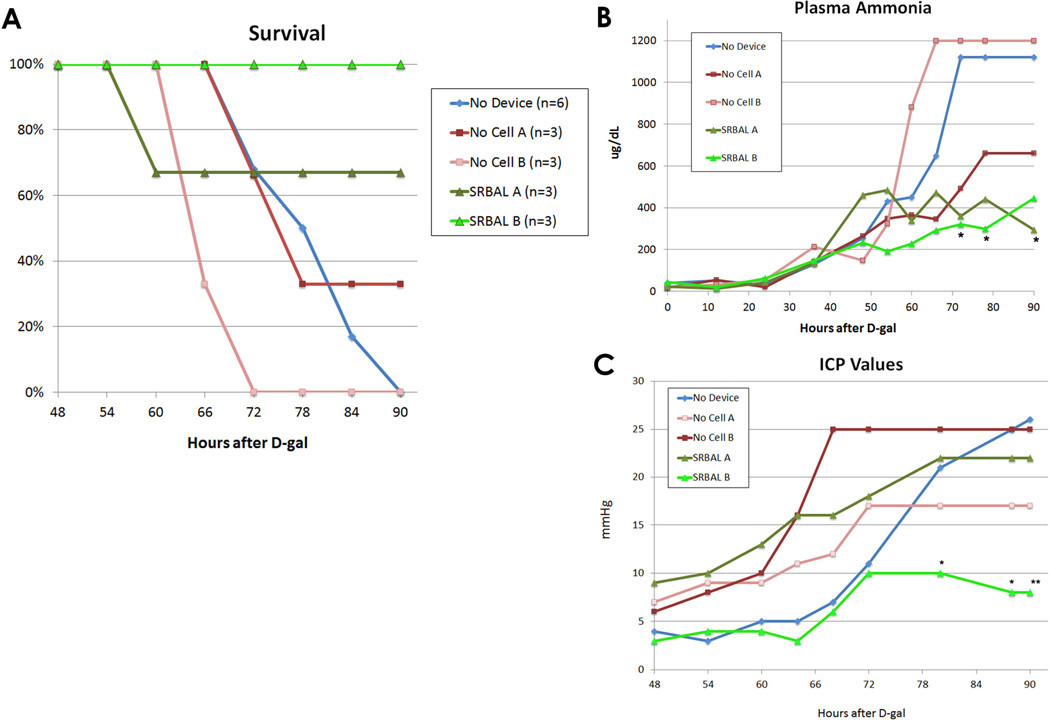
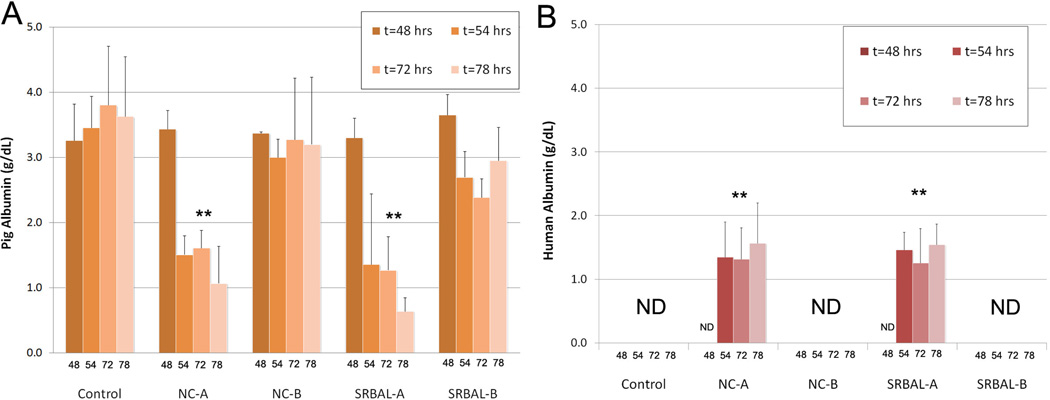
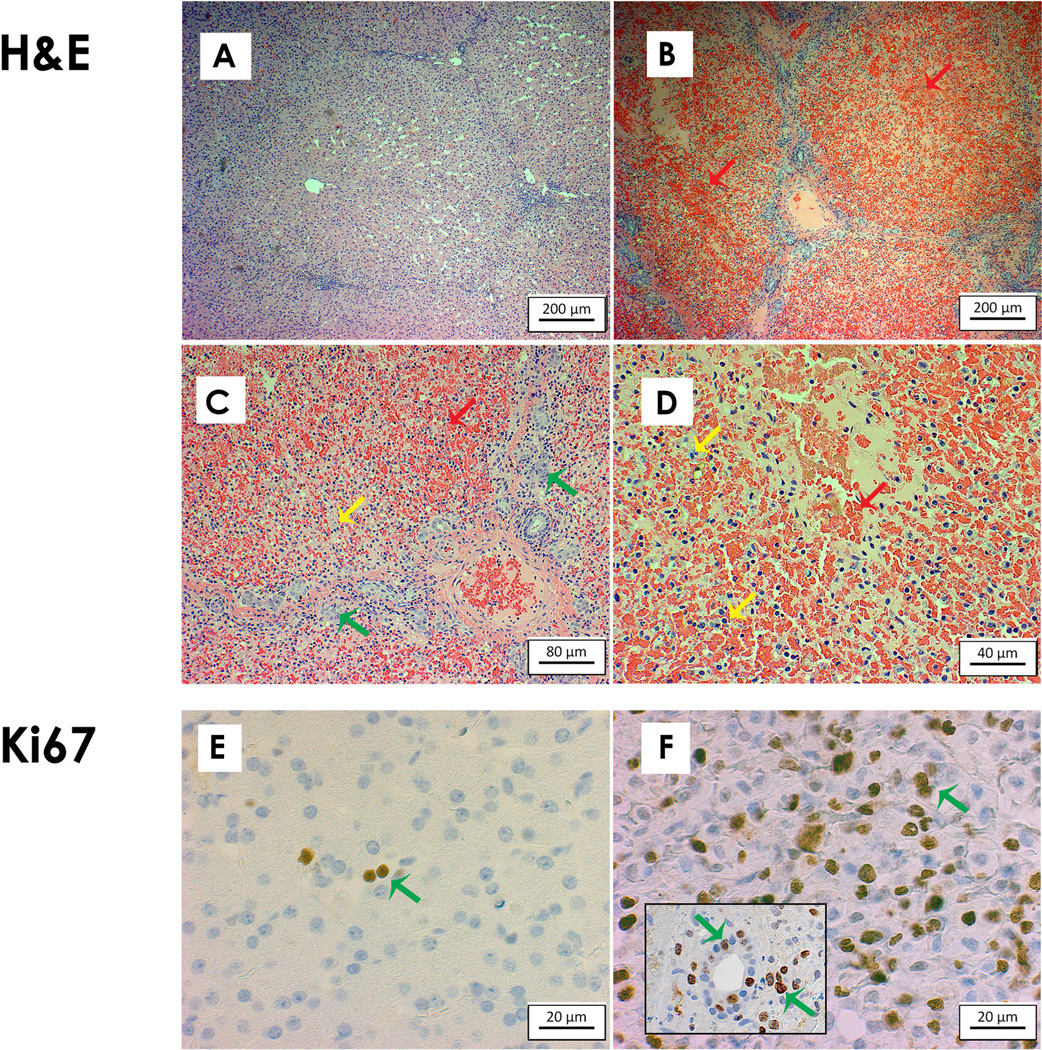
Results: At 48h, all animals had developed encephalopathy and biochemical changes confirming ALF; extracorporeal treatment was initiated and pigs were observed up to 90h after drug infusion. Pigs treated with the SRBAL, loaded with porcine hepatocyte spheroids, had improved survival (83%, n=6) compared to ST alone (0%, n=6, p=0.003) and No-cell device therapy (17%, n=6, p=0.02). Ammonia detoxification, peak levels of serum ammonia and peak ICP, and pig survival were influenced by hepatocyte cell dose, membrane pore size and duration of SRBAL treatment. Hepatocyte spheroids remained highly functional with no decline in mean oxygen consumption from initiation to completion of treatment.
Conclusions: The SRBAL improved survival in an allogeneic model of drug-overdose ALF. Survival correlated with ammonia detoxification and ICP lowering indicating that hepatocyte spheroids prevented the cerebral manifestations of ALF (brain swelling, herniation, death). Further investigation of SRBAL therapy in a clinical setting is warranted.
Keywords: Bioartificial liver; D-galactosamine; Hepatocyte; Liver failure; Spheroid.
Copyright © 2015 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
A new horizon for liver support in acute liver failure.J Hepatol. 2015 Aug;63(2):303-5. doi: 10.1016/j.jhep.2015.05.020. Epub 2015 Jun 2. J Hepatol. 2015. PMID: 26044125 No abstract available.
-
Pivotal preclinical trial of the spheroid reservoir bioartificial liver.J Hepatol. 2015 Oct;63(4):1051-2. doi: 10.1016/j.jhep.2015.06.020. Epub 2015 Jul 2. J Hepatol. 2015. PMID: 26143440 No abstract available.
-
Reply to: "Pivotal preclinical trial of the spheroid reservoir bioartificial liver".J Hepatol. 2015 Oct;63(4):1052-3. doi: 10.1016/j.jhep.2015.06.024. Epub 2015 Jul 2. J Hepatol. 2015. PMID: 26143442 No abstract available.
References
-
- Kjaergard L, Liu J, Als-Nielsen B, al e. Artificial and bioartificial support systems for acute and acute-on-chronic liver failure: a systematic review. JAMA. 2003;289:217–222. - PubMed
-
- Saliba F, Camus C, Durand F, Mathurin P, Letierce A, Delafosse B, Barange K, et al. Albumin dialysis with a noncell artificial liver support device in patients with acute liver failure: a randomized controlled trial. Ann Intern Med. 2013;159:522–531. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
