

Hypercoagulability in dogs with blastomycosis
- PMID: 25818206
- PMCID: PMC4895520
- DOI: 10.1111/jvim.12538
Hypercoagulability in dogs with blastomycosis
Abstract
Background: Blastomycosis is a potentially fatal fungal disease that most commonly affects humans and dogs. The organism causes systemic inflammation and has a predilection for the lungs. The inflammation might lead to a hypercoagulable state with microemboli in the pulmonary circulation which could contribute to inadequate oxygen exchange in infected dogs.
Hypothesis/objectives: Dogs with blastomycosis will be hypercoagulable compared with healthy case-matched controls.
Animals: Client-owned dogs with a diagnosis of blastomycosis (n = 23) and healthy case-matched controls (n = 23).
Methods: Prospective case-controlled study of client-owned dogs presented to a veterinary teaching hospital with clinical signs compatible with blastomycosis. Complete blood counts, fibrinogen, PT, aPTT, thromboelastometry (TE), thrombin antithrombin complexes (TAT), and thrombin generation were evaluated.
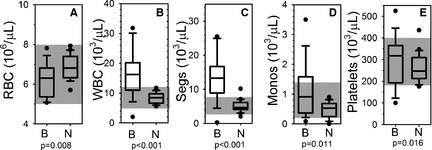
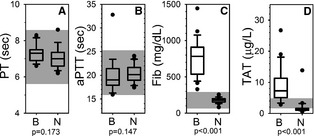
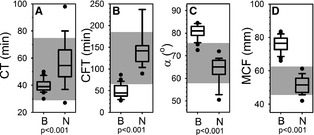
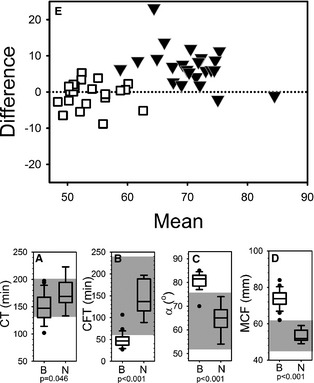
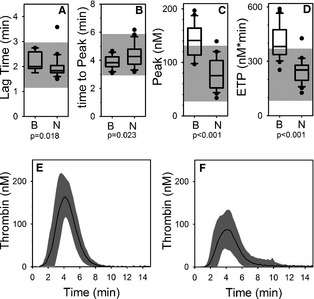
Results: Cases had a leukocytosis compared with controls [mean (SD) 16.6 (7.6) × 10(3)/μL versus 8.2 (1.8) × 10(3)/μL, P < .001], hyperfibrinogenemia [median 784 mg/dL, range 329-1,443 versus median 178 mg/dL, range 82-257, P < .001], and increased TAT concentrations [mean (SD) 9.0 (5.7) μg/L versus 2.0 (2.8) μg/L, P < .001]. As compared to controls, cases were also hypercoagulable as evaluated by thromboelastometry and had increased in vitro thrombin generation on calibrated automated thrombography.
Conclusions and clinical importance: Hypercoagulability occurs in dogs with systemic blastomycosis. Additional studies are needed to explore a possible contribution of thrombogenicity to the clinical manifestations of systemic blastomycosis.
Keywords: Canine; Thromboelastography; Thromboelastometry; Thrombosis.
Copyright © 2015 by the American College of Veterinary Internal Medicine.
Figures
References
-
- Lemos LB, Baliga M, Guo M. Acute respiratory distress syndrome and blastomycosis: Presentation of nine cases and review of the literature. Ann Diagn Pathol 2001;5:1–9. - PubMed
-
- Vasquez JE, Mehta JB, Agrawal R, et al. Blastomycosis in northeast Tennessee. Chest 1998;114:436–443. - PubMed
-
- Chapman SW, Dismukes WE, Proia LA, et al. Clinical practice guidelines for the management of blastomycosis: 2008 update by the Infectious Diseases Society of America. Clin Infect Dis 2008;46:1801–1812. - PubMed
-
- Meyer KC, McManus EJ, Maki DG. Overwhelming pulmonary blastomycosis associated with the adult respiratory distress syndrome. N Engl J Med 1993;329:1231–1236. - PubMed
-
- Gauthier GM, Safdar N, Klein BS, et al. Blastomycosis in solid organ transplant recipients. Transpl Infect Dis 2007;9:310–317. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases